How Effective Are Covid Vaccines, Really?
DEBATES ON COVID - VACCINES, 20 Jun 2022
Swiss Policy Research - TRANSCEND Media Service
Magic potion or snake oil? An honest look at the international data.
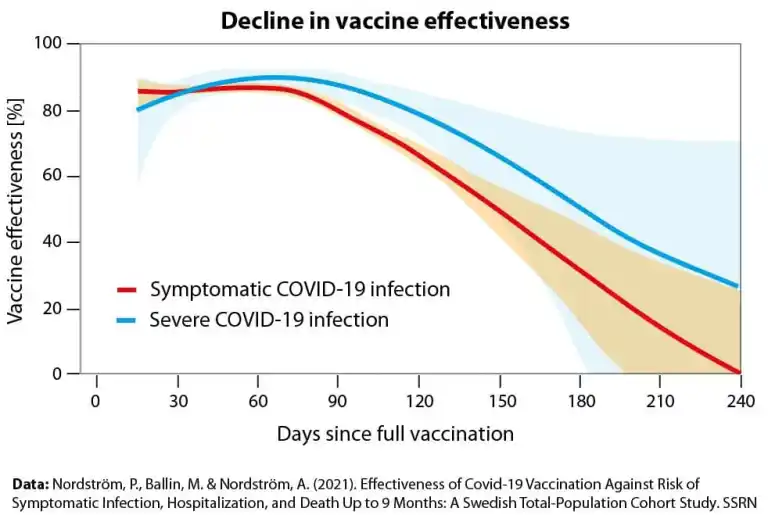
Pre-omicron vaccine protection against infection and severe disease (Nordstroem et al)
Introduction: Different positions towards Covid vaccines
Jun 2022 – There are three different, fundamental positions towards Covid vaccines than can be distinguished:
Positive/promotional: This is the position taken by vaccine manufacturers, many politicians and many (but not all) health agencies. It is typically driven by commercial or political considerations. In addition, many scientists who depend on government or industry money or who want to publish in high-impact journals have also taken a promotional position.
Negative/adverse: This is the position taken by vaccine skeptics. An adverse position can be based on various considerations, such as: 1) a fundamental rejection of vaccines in general; 2) a rejection of Covid vaccines in particular, e.g. due to their novel technology and/or limited trial data; 3) a rejection of vaccines produced by companies with no track record (Moderna, Biontech) or with a criminal track record (Pfizer, Johnson&Johnson, AstraZeneca); 4) or based on strategic considerations (e.g. ‘vaccine passports’ as potential tools of population control).
Neutral / skeptical but open-minded: This is the position taken by some independent investigators and research groups, including Swiss Policy Research. This group of analysts tries to obtain and provide as comprehensive and as nuanced a picture as possible on both vaccine effectiveness and vaccine safety, as well as on strategic considerations.
Different aspects of vaccine protection
In the following analysis, we will distinguish between protection against (symptomatic) infection and protection against severe disease (hospitalization, ICU, death). Furthermore, we will distinguish between the pre-omicron period and the omicron period, and between senior citizens and non-senior citizens. Unless otherwise stated, protection refers to mRNA vaccines (Pfizer, Moderna).
Protection against infection
Prior to omicron (i.e. during the alpha and delta periods), several large studies showed that vaccine protection against symptomatic infection decreased from about 90%/95% shortly after vaccination to close to 0% within about half a year (Lancet). This decrease was first seen in Israel during the delta wave in summer 2021 (SPR).
There have been claims that vaccine protection “turns negative” at some point beyond half a year. However, based on the currently available data, it looks like vaccinated people, who enjoyed a lower infection rate for about half a year, are simply “catching up” with unvaccinated people, but their infection risk is not actually higher than in unvaccinated people without prior infection (which would require some kind of immune suppression). This analysis is backed by the fact that a “booster vaccination” restores protection against infection to the initial level, but again only for a short period of time (Lancet).
Since omicron, vaccine protection against infection starts at 50%-60% shortly after vaccination and decreases to 0% within 4 to 6 months. A booster vaccination restores protection to 50%-60%, but again only for a short period of time. (NEJM)
In contrast to vaccine protection, a previous covid infection confers a more durable protection against re-infection (“natural immunity”). Prior to omicron, a previous covid infection provided 75% to 90% protection against re-infection for over a year, with only a slight decline (JAMA). Since omicron, a non-omicron infection 4 to 12 months earlier still provides a protection of 70% to 50% against re-infection with omicron, according to a study from Qatar (Lancet). According to a study from Denmark, which included more older people, protection decreased from 50% to 20% for a previous infection 6 months to 12+ months ago (Lancet).
Furthermore, it has been shown that viral load and infectiousness are identical in unvaccinated and in vaccinated people (once infection occurs) (medRxiv). In addition, there is no strong evidence that vaccination reduces the risk of mild or moderate covid (once infection occurs), contrary to countless claims on Twitter (“grateful to be vaccinated and boosted”). In other words, covid vaccination cannot prevent mild to moderate covid infection. There is also no strong evidence that vaccination reduces the risk of long covid in non-senior citizens (Nature).
Concerning negative vaccine protection, there is one important exception: for about 7 to 10 days immediately after vaccination – especially after the first vaccination and apparently also after a later “booster vaccination” – the risk of infection is indeed increased, possibly due to the known, transient immune suppression (lymphocytopenia) and increased exposure (“post-vaccination spike”). This effect is important because it looks like in several countries, mass vaccination campaigns have indeed triggered new covid waves or amplified ongoing covid waves (if the vaccination campaign was running in parallel to such a wave, e.g. in Israel).
In sum, the fact that current covid vaccines provide only short-term, rapidly waning protection against infection and transmission means that covid vaccines do not contribute to infection control, neither at the individual level nor at the population level. However, contrary to claims by skeptics, there is also currently no evidence that vaccination increases infection rates (with the exception of the post-vaccination spike mentioned above). Rather, covid waves, similar to flu waves, oscillate at global and continental scales (e.g. between Western and Eastern Europe).
The fact that vaccine protection against infection and transmission is waning rapidly means that so-called “vaccine passports” are epidemiologically inappropriate or indeed counterproductive. For the same reason, vaccine mandates, even in health care workers, are medically unjustified. Based on Israeli data from early summer 2021, these facts had already been known before most countries even introduced such schemes.
Nevertheless, covid vaccines may provide protection against severe disease and death in high-risk groups. This question will be discussed in the next section.
Protection against severe disease and death
Prior to omicron, vaccine protection against severe disease in senior citizens (hospitalization, ICU and death) decreased from about 95% to about 60% within half a year (Lancet). It was this decrease that triggered the first booster campaigns, beginning in Israel in the summer of 2021. In younger people, the protection was somewhat more durable (about 80% after half a year) (Lancet).
The omicron variant has achieved substantial immune escape, and neutralization power of existing vaccines, which are still based on the spike protein of the original 2019 Wuhan variant, decreased by a factor of 10 to 50 compared to previous variants (SPR). Initially, it was uncertain if current vaccines would still provide any protection against omicron infection and severe disease.
Nevertheless, an analysis from Taiwan, which had almost no covid infections before experiencing a massive omicron wave in the spring of 2022, shows that in senior citizens (70+), a recent booster vaccination provides about 75% to 80% protection against death; in contrast, double vaccination (several months ago) provides only about 40% protection against death (TCDC).
Similarly, a British study on the risk of omicron hospitalization found that double vaccination months ago provided about 40% protection and a recent booster about 60% to 80% protection (Lancet). Clearly, the decisive point is not the number of vaccinations, but rather the time since the last vaccination (as is the case with flu vaccination).
A recent study from Qatar found higher values: two doses several months ago provided about 75% protection against severe disease or death, whereas a booster a few weeks ago provided about 90% protection. However, in the Qatar study, only 2% of participants were over 70 years of age, i.e. these results are not directly applicable to Western or East Asian populations. (NEJM)
Thus, it looks like against omicron, vaccination several months ago reduces the risk of severe disease by about 50%, while recent vaccination may reduce the risk by about 75% (in senior citizens). It is possible that this continuing protection is due to a combination of limited levels of neutralizing antibodies, non-neutralizing antibodies, and the T-cell response (NIH).
In comparison, natural immunity from a previous infection (without any vaccination) provides more durable protection against severe disease upon reinfection. Prior to omicron, studies found a protection against hospitalization of about 90% for over a year with no declining trend (JAMA). Against omicron, the Qatar study, which included mostly young people, found a protection of 75% to 95% (NEJM). The important question of how strongly a previous (non-omicron) infection protects against severe omicron disease in senior citizens has not yet been answered.
Concerning vaccine protection against severe disease, the decreasing immune response with age (so-called immunosenescence) is of importance. Most vaccine studies did not include very old citizens (80+) or nursing home residents, despite the fact that these are the groups most at risk of severe covid. Already in early 2021, studies showed that one third of people over 80 did not develop any neutralizing antibodies in response to covid vaccination, and that in nursing homes residents, vaccine protection against infection reached at most 65%. (SPR)
This fact is important when analyzing country-level data, as will be done in the next section.
Country analyses
Vaccine study data reviewed above suggested that since omicron, protection against infection starts at 50% and drops to zero within a few months, whereas protection against severe disease and death in senior citizens starts at 75% and decreases to 50% within a few months. Are these values consistent with what has been observed in various Western and Asian countries?
The analysis of vaccine protection against omicron is complicated by the fact that in terms of hospitalizations and deaths, the omicron variant itself is about 60% to 80% milder compared to previous variants (Lancet). Furthermore, the mildness and very rapid spread of omicron means that 50% to 70% of PCR+ hospitalizations and deaths are just “with covid”, not “from covid”, compared to about 10% to 20% during previous covid waves (SSI). Finally, the fact that many people already had a previous covid infection further adds to the complexity of calculating vaccine protection.
Even excess mortality data can be difficult to interpret due to pandemic and lockdown-related non-covid deaths (e.g. from cancer and heart disease), a return of strong flu waves in several countries, potential vaccine deaths, and seasonal factors (e.g. an out-of-season covid wave causes higher relative excess mortality than a seasonal wave).
Nevertheless, it is worth taking a look at real-world data from some notable countries.
Switzerland: Switzerland is an interesting case because it is the only country that has been using mainly the high-dosed Moderna vaccine (40% Moderna, 25% Pfizer, 30% unvaccinated). Swiss authorities provide detailed covid hospitalization and death data per age group and vaccination status (BAG, in English). Thus, one can see that during the two omicron waves in January and March 2022, double-vaccination provided still about 60% protection and recent booster vaccination provided about 90% to 80% protection against severe disease in senior citizens. Furthermore, Moderna provided consistently higher protection compared to Pfizer.
Hong Kong: Hong Kong is another fascinating case, as it had almost no infections for two years but then experienced a record-breaking omicron wave in February/March 2022 with very high covid death figures. At first glance this looked like total vaccine failure, but a closer inspection showed that vaccination rates in senior citizens were only 30% to 50%; 60% of deaths occurred in nursing homes; 90% of deaths were not yet double-vaccinated; and excess mortality was only about 65% of covid mortality (i.e. a third of PCR+ deaths weren’t actually covid deaths).
A comparison with Taiwan (80% booster rate in senior citizens (TCDC)) shows that the omicron wave in Taiwan reached about 40% of peak infections, but only 20% of peak deaths compared to Hong Kong (OWD). Thus, the case of Hong Kong does not contradict vaccine protection.
Australia: Due to strict border controls, Australia largely avoided pre-omicron infection waves, but the country has experienced several large omicron waves from January to June 2022. Compared to Hong Kong, total cases stand at 200%, but total deaths stand at only 30% (despite a much higher obesity rate in Australia) (OWD). Compared to the UK, total Australian PCR cases currently stand at 90%, but total PCR+ deaths stand at only 15% (per capita). Thus, Australian data, too, appears to be consistent with continuing vaccine protection in senior citizens.
Israel: Covid vaccination pioneer Israel is the only European country that suffered higher excess mortality during the first omicron wave than during previous waves (EuroMomo). Nevertheless, official Israeli data shows that during the omicron wave, recently vaccinated senior citizens (3rd or 4th dose) had a 90% lower risk of severe disease, and senior citizens vaccinated a few months ago still had a 50% lower risk compared to unvaccinated citizens (IMH). The Israeli omicron wave was ten times higher than any previous wave in Israel, and it was higher even than the omicron wave in Hong Kong one month later (OWD). It is possible that the Israeli wave was so explosive because Israel once again vaccinated right into an ongoing wave.
In conclusion, one can see that real-world data from several countries are consistent with a short-term vaccine protection against severe disease in the range of 50% to 90%.
Nevertheless, even highly vaccinated populations continue to see non-trivial levels of covid disease. This is likely because of several factors: first, vaccination simply cannot limit transmission; second, vaccine protection against severe disease is typically only twofold to five-fold (50% to 80%) and not twenty-fold (95%); and third, omicron, although milder, has produced unprecedented infection rates (ten times higher than during previous waves).
Updated vaccines and antigenic priming
Will updated omicron vaccines improve protection against omicron infection and disease? It looks like this is not going to be the case, as prior vaccination or prior infection has “primed” the immune response to the pre-omicron virus or spike protein, and an updated vaccine can no longer significantly change the immune response (so-called antigenic priming) (Nature).
Moderna recently reported that its updated omicron vaccine increased neutralizing antibodies against omicron by a factor of 8, but a factor of 8 is very low (not even one order of magnitude), especially since the baseline was very low already, and it only applies to people without any prior infection, which by now is a small minority (Moderna).
It has also been shown that vaccinated people, once infected, often produce antibodies only against the spike (S) protein (as induced by the vaccine), but not against the nucleocapsid (N) protein of the virus, in contrast to unvaccinated people (NIH). The significance of this limited immune response in vaccinated people is not yet clear, as anti-N antibodies are not neutralizing antibodies, and children often do not produce anti-N antibodies, either (Nature). Anti-N antibodies could be beneficial, irrelevant, or even detrimental against future variants and infections.
In sum, it looks like SARS-CoV-2 antigenic priming now is a reality, both in vaccinated and in previously infected people, and current vaccine products are unlikely to significantly improve their effectiveness against future variants. On the other hand, there is still no evidence of antibody-dependent enhancement (ADE) of covid infection or disease.
Distorting vaccine protection
Vaccine protection can be exaggerated (by vaccine promoters) or downplayed (by vaccine skeptics).
Typical methods to exaggerate vaccine protection are: 1) not counting infections shortly after vaccination (“vaccinated” vs. “injected”); 2) counting patients with missing vaccination data as “unvaccinated”; 3) using outdated population data to exaggerate infections and hospitalizations in the unvaccinated.
Typical methods to downplay vaccine protection are: 1) Ignoring infection rates when comparing death rates; 2) confounding age groups; 3) comparing vaccinated to recovered people instead of unexposed people (“negative protection”); 4) not distinguishing between with/from covid (especially since omicron).
Vaccine skeptics have correctly pointed out that in addition to relative effectiveness, one should also consider absolute effectiveness, which strongly depends on age. For instance, a 90% relative effectiveness translates into a an absolute reduction of pre-omicron covid lethality from 1% to 0.1% (i.e. –0.9%) in senior citizens (outside of nursing homes) and from 0.05% to 0.005% in 45-year-old people (i.e. –0.045%) (SPR).
Vaccine injuries
While the current review has focused on vaccine protection only, it should be recalled that covid vaccines are first-generation investigational vaccines with controversial short-term safety data, especially in young people, and still unknown long-term safety data.
Indeed, in several countries authorization of some covid vaccine brands has already been denied, withdrawn, or limited to certain age groups due to significant safety signals. Serious vaccine adverse events include cardiovascular, neurological and immunological conditions. Additional booster vaccinations could further increase covid vaccine adverse events.
Read more: Covid Vaccine Adverse Events: An Overview (SPR)
Conclusion
Both vaccine study data and real-world data reviewed above suggest that since omicron, vaccine protection against infection starts at 50% and drops to zero within a few months, whereas protection against severe disease and death in senior citizens starts at 75% and decreases to 50% within a few months.
Furthermore, there is no difference in viral load and infectiousness between vaccinated and unvaccinated people; no evidence that vaccination reduces the risk of mild or moderate covid; and no evidence that vaccination reduces the risk of long covid in non-senior citizens. Prior covid infection continues to provide a more durable protection against re-infection.
Thus, while the risk/benefit ratio may still positive in senior citizens and other risk groups (based on current evidence), this does not appear to be the case in healthy young adults and children. Danish professor in global health and vaccine expert, Dr. Christine Stabell-Benn, recently argued that she “wouldn’t recommend vaccination of anybody under 50 years of age.”
Furthermore, both “vaccine passports” and vaccine mandates, even for health care workers, have no medical or epidemiological justification and should be abandoned.
Figures:
1) Taiwan: Vaccine protection against death during the omicron wave

2) Pre-omicron vaccine protection against infection and severe covid (Sweden)

3) Switzerland: Vaccine protection against hospitalization (70-79)

4) Qatar (only 2% over 70): Previous infection and vaccination against omicron infection

5) Same viral load in vaccinated and unvaccinated people (delta)

See also
__________________________________________
![]() Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Tags: COVID-19, Vaccines
DISCLAIMER: The statements, views and opinions expressed in pieces republished here are solely those of the authors and do not necessarily represent those of TMS. In accordance with title 17 U.S.C. section 107, this material is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. TMS has no affiliation whatsoever with the originator of this article nor is TMS endorsed or sponsored by the originator. “GO TO ORIGINAL” links are provided as a convenience to our readers and allow for verification of authenticity. However, as originating pages are often updated by their originating host sites, the versions posted may not match the versions our readers view when clicking the “GO TO ORIGINAL” links. This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more information go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
One Response to “How Effective Are Covid Vaccines, Really?”
Read more
Click here to go to the current weekly digest or pick another article:
DEBATES ON COVID - VACCINES:
I would like to pose a question about PCR testing. Early PCR testing and even now in some areas the amount of ‘spinning’ 20-30-40 cycles in some cases to detect covid effects. Wouldn’t high replication results in detection of any previous corona virus in a patient dramatically sku any results of accrued data? Would it not increase reports of covid 19 sars 2 infection where no infection truly existed?