
The Ivermectin Debate
COVID19 - CORONAVIRUS, 26 Jul 2021
Swiss Policy Research - TRANSCEND Media Service
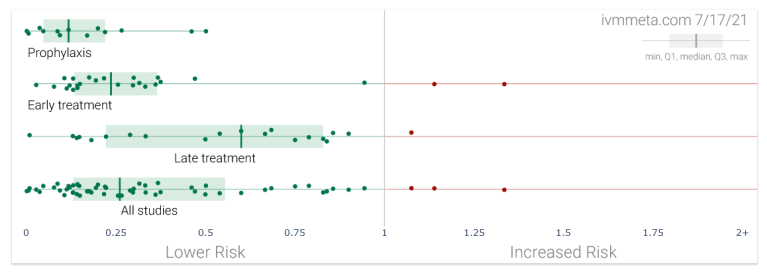
Ivermectin against covid: study results by treatment stage (IVMMETA)
Is Ivermectin highly effective or totally useless against covid? And why is there still no agreement on this question?
Please note: Patients are asked to consult a doctor.
25 Jul 2021 – To date, about 50 studies – among them about 30 randomized controlled trials and about 40 peer-reviewed publications – have been done on the use of ivermectin against covid. Most of these studies found that the use of ivermectin was associated with a positive outcome, such as a reduced risk of infection, hospitalization or death (see chart above; not all of these results were significant).
Based on these studies, several meta-analyses computed positive results, too. Most recently, a WHO-supported meta-analysis of 24 randomized controlled trials found a 56% mortality reduction overall and a 70% mortality reduction in patients who received early outpatient treatment. There even appears to be a positive dose-response relationship, which is another indicator of effectiveness.
Nevertheless, several concerns have been raised regarding the reliability of these results, and major – although not necessarily “independent” – health authorities like the WHO, the US FDA and the European EMA all continue to advise against the use of ivermectin outside of clinical trials.
First, it has been argued that there might be some publication bias, that is, only positive studies may have been published, while negative studies may have remained unpublished. However, the above mentioned meta-analysis was able to show that there is in fact no publication bias: studies that had been registered or announced did indeed get published, at least as a pre-print.
But secondly, and more importantly, it has been argued that many of the existing studies are of rather low quality: due to budget constraints, many of them are small, single-center, open-label (not double-blinded) and not perfectly randomized, thus significantly reducing their reliability. It is possible that many of these studies were biased towards getting a positive result.
Thirdly, and most worryingly, some of these studies may simply be fraudulent or fake. As a matter of fact, one of the first positive studies on ivermectin, published in mid-April 2020, was from the very same group (Surgisphere) that published a fraudulent (negative) study on HCQ in the Lancet (both studies were ultimately retracted). And just last week, another seemingly positive study on ivermectin by an Egyptian group was shown to be very likely fraudulent.
It remains debatable whether the groups behind these fraudulent studies simply tried to jump on the bandwagon of a promising medication, or if their role was in fact more substantial. In a context unrelated to ivermectin and covid, a former editor of the British Medical Journal recently argued that “we have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary.”
Finally, and contrary to what some ivermectin proponents have argued, the epidemiological evidence in favor of ivermectin is rather weak. Ivermectin hasn’t “crushed the curve” anywhere; rather, decreases in infections were mostly driven by seasonal and endemic effects. In fact, ivermectin pioneers like Peru and Mexico have some of the highest covid mortality rates in the world; to their defense, even in Latin America, ivermectin use has often been limited and local.
On the other hand, the few studies claiming that ivermectin did not work against covid are also of rather low or dubious quality. The most famous one – a Colombian trial published in JAMA – was done so poorly that over 100 scientists and doctors called for its retraction. Furthermore, the only negative meta-analysis simply excluded most positive trials, confused the control and treatment group of another trial, and made several statistical mistakes, also triggering calls for retraction.
Most recently, a detailed covid animal study by the renowned French Institute Pasteur found that ivermectin “limited inflammation and prevented clinical deterioration”, but did not reduce viral load. The study “supports the use of ivermectin as an immuno-modulatory drug in covid patients”, but it would also, if applicable to humans, directly question the validity of several studies that claimed ivermectin works as an anti-viral prophylaxis against coronavirus infection.
To resolve this situation and finally answer the question of the effectiveness of ivermectin against covid, several high-quality randomized controlled trials (RCTs) are currently ongoing, sponsored by large foundations or public funds. While rather late in the pandemic, these trials are certainly of crucial importance to settle the ivermectin debate.
Large and expensive RCTs may, however, come with their own intricacies, as was most recently seen in the case of the covid vaccine trials. Specifically, RCTs may to some extent be “designed to succeed” or “designed to fail”. In the case of covid – a multi-phasic disease with a very steep age-based risk gradient – a trial can be designed to fail by enrolling (young) low-risk participants, using drugs late instead of early, under-dose or in some cases even over-dose the drug.
For instance, the ongoing TOGETHER trial of ivermectin, sponsored by the Gates Foundation, was caught using just a single dose of ivermectin, whereas successful trials used two to four doses per day for up to five days. The Oxford PRINCIPLE trial, meanwhile, was caught enrolling participants up to 15 days after symptom onset, at which point some high-risk covid patients are already dead. The Oxford group had previously “botched” several other early treatment trials.
An even deeper issue, however, is that almost all covid medication trials have been looking for a single “wonder drug”, whereas it is increasingly clear that severe covid really is an auto-immune, hyper-inflammatory and pro-thrombotic condition, which in high-risk patients may have to be treated by a combination of drugs (and as early as possible). This is becoming all the more important as the long-term protection by covid vaccines appears to fall increasingly short of expectations.
In conclusion, the current evidence base concerning the use of ivermectin in the early treatment of covid continues to be positive, but important questions regarding the quality and certainty of many studies remain. It is to be hoped that ongoing high-quality RCTs will be able to resolve the debate. Given a still rising global covid mortality of currently about ten million people, if ivermectin is even just 10% effective against covid, its professional use could already have saved a million people.
See also: What’s the deal with Ivermectin and COVID? (Interview)
Related
__________________________________________
![]() Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Tags: COVID-19, Coronavirus, Ivermectin, Pandemic, Vaccines
DISCLAIMER: The statements, views and opinions expressed in pieces republished here are solely those of the authors and do not necessarily represent those of TMS. In accordance with title 17 U.S.C. section 107, this material is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. TMS has no affiliation whatsoever with the originator of this article nor is TMS endorsed or sponsored by the originator. “GO TO ORIGINAL” links are provided as a convenience to our readers and allow for verification of authenticity. However, as originating pages are often updated by their originating host sites, the versions posted may not match the versions our readers view when clicking the “GO TO ORIGINAL” links. This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more information go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
Read more
Click here to go to the current weekly digest or pick another article:
COVID19 - CORONAVIRUS: