What if PTSD Is More Physical Than Psychological?
MILITARISM, 13 Jun 2016
Robert F. Worth – The New York Times Magazine
A new study supports what a small group of military researchers has suspected for decades: that modern warfare destroys the brain.

Brandon Matthews, a former Army Ranger who was exposed to a series of blasts while serving in Iraq and elsewhere and now suffers from cognitive problems.
Nick Oza for The New York Times
10 Jun 2016 – In early 2012, a neuropathologist named Daniel Perl was examining a slide of human brain tissue when he saw something odd and unfamiliar in the wormlike squiggles and folds. It looked like brown dust; a distinctive pattern of tiny scars. Perl was intrigued. At 69, he had examined 20,000 brains over a four-decade career, focusing mostly on Alzheimer’s and other degenerative disorders. He had peered through his microscope at countless malformed proteins and twisted axons. He knew as much about the biology of brain disease as just about anyone on earth. But he had never seen anything like this.
The brain under Perl’s microscope belonged to an American soldier who had been five feet away when a suicide bomber detonated his belt of explosives in 2009. The soldier survived the blast, thanks to his body armor, but died two years later of an apparent drug overdose after suffering symptoms that have become the hallmark of the recent wars in Iraq and Afghanistan: memory loss, cognitive problems, inability to sleep and profound, often suicidal depression. Nearly 350,000 service members have been given a diagnosis of traumatic brain injury over the past 15 years, many of them from blast exposure. The real number is likely to be much higher, because so many who have enlisted are too proud to report a wound that remains invisible.
For years, many scientists have assumed that explosive blasts affect the brain in much the same way as concussions from football or car accidents. Perl himself was a leading researcher on chronic traumatic encephalopathy, or C.T.E., which has caused dementia in N.F.L. players. Several veterans who died after suffering blast wounds have in fact developed C.T.E. But those veterans had other, nonblast injuries too. No one had done a systematic post-mortem study of blast-injured troops. That was exactly what the Pentagon asked Perl to do in 2010, offering him access to the brains they had gathered for research. It was a rare opportunity, and Perl left his post as director of neuropathology at the medical school at Mount Sinai to come to Washington.
Perl and his lab colleagues recognized that the injury that they were looking at was nothing like concussion. The hallmark of C.T.E. is an abnormal protein called tau, which builds up, usually over years, throughout the cerebral cortex but especially in the temporal lobes, visible across the stained tissue like brown mold. What they found in these traumatic-brain-injury cases was totally different: a dustlike scarring, often at the border between gray matter (where synapses reside) and the white matter that interconnects it. Over the following months, Perl and his team examined several more brains of service members who died well after their blast exposure, including a highly decorated Special Operations Forces soldier who committed suicide. All of them had the same pattern of scarring in the same places, which appeared to correspond to the brain’s centers for sleep, cognition and other classic brain-injury trouble spots.
Then came an even more surprising discovery. They examined the brains of two veterans who died just days after their blast exposure and found embryonic versions of the same injury, in the same areas, and the development of the injuries seemed to match the time elapsed since the blast event. Perl and his team then compared the damaged brains with those of people who suffered ordinary concussions and others who had drug addictions (which can also cause visible brain changes) and a final group with no injuries at all. No one in these post-mortem control groups had the brown-dust pattern.
Perl’s findings, published in the scientific journal The Lancet Neurology, may represent the key to a medical mystery first glimpsed a century ago in the trenches of World War I. It was first known as shell shock, then combat fatigue and finally PTSD, and in each case, it was almost universally understood as a psychic rather than a physical affliction. Only in the past decade or so did an elite group of neurologists, physicists and senior officers begin pushing back at a military leadership that had long told recruits with these wounds to “deal with it,” fed them pills and sent them back into battle.
If Perl’s discovery is confirmed by other scientists — and if one of blast’s short-term signatures is indeed a pattern of scarring in the brain — then the implications for the military and for society at large could be vast. Much of what has passed for emotional trauma may be reinterpreted, and many veterans may step forward to demand recognition of an injury that cannot be definitively diagnosed until after death. There will be calls for more research, for drug trials, for better helmets and for expanded veteran care. But these palliatives are unlikely to erase the crude message that lurks, unavoidable, behind Perl’s discovery: Modern warfare destroys your brain.
The physics behind blast forces was almost unknown until the modern era, and it remains so mysterious and terrifying that scientists sometimes invoke the word “magic” when talking about it. A blast begins simply: A detonator turns a lump of solid matter into a deadly fireball. Within that moment, three distinct things happen. The first is the blast wave, a wall of static pressure traveling outward in all directions faster than the speed of sound. Next, a blast wind fills the void and carries with it any objects it encounters. This is the most manifestly destructive part of the blast, capable of hurling cars, people and shrapnel against buildings and roadsides. The remaining effects include fire and toxic gases, which can sear, poison and asphyxiate anyone within range.
The effects of all of this on the human body are myriad and more complicated than the blast itself. People who have been exposed to blasts at close range usually describe it as an overpowering, full-body experience unlike anything they have ever known. Many soldiers do not recall the moment of impact: it gets lost in the flash of light, the deafening sound or unconsciousness. Those who do remember it often speak of a simultaneous punching and squeezing effect, a feeling at once generalized and intensely violent, as if someone had put a board against your body and then struck it with dozens of hammers. From a distance, a blast makes a distinctive thump, the sound of air pressure clapping outward. When I lived in Baghdad, reporting for this newspaper, I would sometimes be awakened by that sound early in the morning. I would sit up in bed, instantly alert, with a surreal and awful realization: Someone who was just as healthy as me 30 seconds ago has been shredded to pieces.
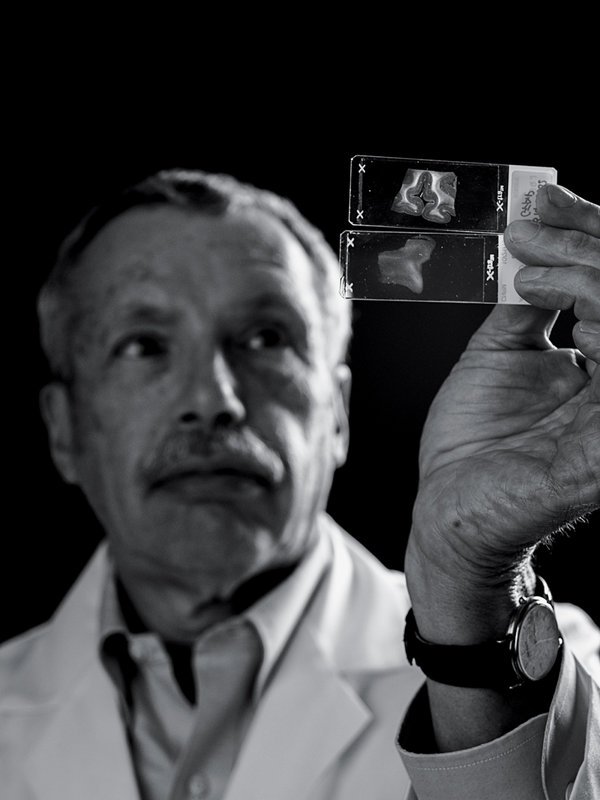
Dr. Daniel Perl holds a slide with brain tissue (top) that shows signs of a blast injury. The other slide shows a healthy brain.
Greg Kahn for The New York Times
Trinitrotoluene, or TNT, was first used in artillery shells by the German Army in 1902. Soon after the First World War started in 1914, a rain of these devices was falling on the hapless men on each side of the front. It was a level of violence and horror far beyond the cavalry charges of earlier wars. Very quickly, soldiers began emerging with bizarre symptoms; they shuddered and gibbered or became unable to speak at all. Many observers were struck by the apparent capacity of these blasts to kill and maim without leaving any visible trace. The British journalist Ellis Ashmead-Bartlett famously described the sight of seven Turks at Gallipoli in 1915, sitting together with their rifles across their knees: “One man has his arm across the neck of his friend and a smile on his face as if they had been cracking a joke when death overwhelmed them. All now have the appearance of being merely asleep; for of the several I can only see one who shows any outward injury.”
For those who survived a blast and suffered the mysterious symptoms, soldiers quickly coined their own phrase: shell shock. One period lyric went like this:
Perhaps you’re broke and paralyzed
Perhaps your memory goes
But it’s only just called shell shock
For you’ve nothing there that shows.
One British doctor, Frederick Mott, believed the shock was caused by a physical wound and proposed dissecting the brains of men who suffered from it. He even had some prescient hunches about the mechanism of blast’s effects: the compression wave, the concussion and the toxic gases. In a paper published in The Lancet in February 1916, he posited a “physical or chemical change and a break in the links of the chain of neurons which subserve a particular function.” Mott might not have seen anything abnormal in the soldiers’ brains, even if he had examined them under a microscope; neuropathology was still in its infancy. But his prophetic intuitions made him something of a hero to Perl.
Mott’s views were soon eclipsed by those of other doctors who saw shell shock more as a matter of emotional trauma. This was partly a function of the intellectual climate; Freud and other early psychologists had recently begun sketching provocative new ideas about how the mind responds to stress. Soldiers suffering from shell shock were often described as possessing “a neuropathic tendency or inheritance” or even a lack of manly vigor and patriotic spirit. Many shell-shock victims were derided as shirkers; some were even sentenced to death by firing squad after fleeing the field in a state of mental confusion.
This consensus held sway for decades, even as the terminology shifted, settling in 1980 on “post-traumatic stress disorder,” a coinage tailored to the unique social and emotional strain of returning veterans of the war in Vietnam. No one doubted that blasts had powerful and mysterious effects on the body, and starting in 1951, the U.S. government established the Blast Overpressure Program to observe the effects of large explosions, including atomic bombs, on living tissue. One of my uncles recalls standing in the Nevada desert as an Army private in 1955, taking photographs of a nuclear blast amid a weird landscape of test objects: cars, houses and mannequins in Chinese and Soviet military uniforms. At the time, scientists believed blasts would mainly affect air pockets in the body like the lungs, the digestive system and the ears. Few asked what it would mean for the body’s most complex and vulnerable organ.
Only after yet another European war broke out did scientists begin looking again at blast’s effects on the brain. When the Balkans collapsed into fratricidal violence in the early 1990s, Ibolja Cernak, a small, tenacious woman who grew up in the countryside of what is now Serbia, was working as a doctor and researcher at a military hospital in Belgrade. She soon began seeing large numbers of soldiers with blast trauma, usually from mortars and artillery fire, a common feature of that war. As in World War I, the men often suffered from striking mental impairments but few visible wounds. Cernak, whose colleagues call her Ibi, has an appealing blend of briskness and warmth, along with a clinician’s conviction that you must listen to your patients. It is easy to imagine her running around the battlefields of Bosnia and Serbia, collecting blood samples from soldiers. That is what she did for several years, at no small risk to her life, for a study cataloging the neurological effects of blast on 1,300 recruits. “The blast covers the entire body,” she told me. “It has a squeezing effect. Ask soldiers what they felt: The first thing they say is that their ears were popped out, they were gasping for air, like some huge fist is squeezing them. The entire body is involved in that interaction.”
Cernak became convinced that blast ripples through the body like rings on a pond’s surface. Its speed changes when it encounters materials of different density, like air pockets or the border between the brain’s gray and white matter, and can inflict greater damage in those places. As it happens, physicists would later theorize some very similar models for how blast damages the brain. Several possibilities have now been explored, including surges of blood upward from the chest; shearing loads on brain tissue; and the brain bouncing back and forth inside the skull, as happens with concussion. Charles Needham, a renowned authority on blast physics, told me post-mortems on blast injuries have lent some support to all of those theories, and the truth may be that several are at play simultaneously.
A decade after her initial battlefield surveys in the Balkans, Cernak took a position at Johns Hopkins University in Baltimore, where she did animal research that bolstered her conviction about blast’s full-body effects. She found that even if an animal’s head is protected during a blast, the brain can sustain damage, because the blast wave transfers through the body via blood and tissue. Cernak also came to believe that blast injuries to the brain were cumulative and that even small explosions with no discernible effects could, if repeated, produce terrible and irreversible damage. Much of this would later be confirmed by other scientists.
Even Cernak’s limited conclusions about blast injuries were heresy to much of the military-medical establishment at the time. She presented some of her findings at a conference in Vienna in the late 1990s, and before she was even finished, “an older gentleman stood up, a military doctor from the U.S.A.,” she recalled. “He said: ‘Stop with this nonsense. If you give soldiers fluid replacement, they’ll do fine after 24 hours, so it’s not this.’ … I was taken aback. It’s been an uphill battle.”

Australian soldiers in a field hospital near Ypres, Belgium, during World War I, when “shell shock” was first noted.
Australian War Memorial
It was not until 2001, when America embarked on what became an era of constant warfare, that doctors began to move slowly toward Cernak’s way of thinking. A new generation of more powerful roadside bombs — improvised explosive devices, or I.E.D.s, in military parlance — became a signature of the fighting in Iraq and Afghanistan, yielding an epidemic of blast injury. Medics soon noticed an oddity of blast: It reflects off hard surfaces and multiplies, so that people who appear to be protected inside an enclosed space like a Humvee often suffer much worse brain injuries than those outside. Military and civilian researchers began focusing their work on the brain rather than just the body. But it was still very difficult to isolate blast from all the other physical and mental effects of being exposed to an explosion in a combat zone.
A landmark advance came in 2007, when an engineering firm called Applied Research Associates received a call from the SWAT team of the Arapahoe County Sheriff’s Office in Colorado. The officers were worried about possible neurological effects from breaching, the practice of blowing open doors with small explosive charges. Almost every major city in the United States has breacher teams, as do militaries in war zones. The Applied Research team quickly recognized that monitoring breachers would allow them to observe blast in its pure form, because the charges are too small to knock soldiers over or give them concussions; they are subject to the blast wave only. Plus, the researchers could bypass any ethical concerns about running tests on human subjects, because the breachers were doing it anyway.
The Applied Research team quickly designed and led a study on military breachers, rigging its own blast gauges and subjecting the recruits and trainers to neuropsychological tests at the beginning and end of a two-week breaching course. The resulting report, circulated in 2008, found a small but distinct decline in performance among the instructors, who are exposed to far more blasts than students. It was only a pilot study, but one author, Leanne Young, told me it added to “converging evidence that there is a cumulative effect with chronic exposure to blast,” even at relatively low levels.
The military was still reluctant to take blast seriously or even to concede that the symptoms it caused were a matter of physical harm. As late as 2008, researchers at the Walter Reed Army Institute of Research published a paper suggesting that the symptoms of traumatic brain injury could be caused in large part by PTSD and brushing off “theoretical concern” about neurological effects of the blast wave. By that time, American doctors who had gained Cernak’s unusual blend of medical expertise and battle experience were starting to draw their own conclusions.
One of the first to challenge the military from within was a 44-year-old Army lieutenant colonel named Christian Macedonia. In March 2008, Macedonia was in Arlington, Va., listening to a group of scientists and government bureaucrats talk about roadside bombs. The talk was dry and technical, and finally Macedonia, a square-jawed man with an air of urgent candor, could no longer contain himself. He lashed out against the military’s inaction on brain injury, using what he recalls as “some pretty salty language” to make his point. “I see no movement, and I’m kind of sick of it,” he concluded. As the meeting broke up, Macedonia expected other participants to politely avoid him. Instead, a younger aide approached, gave him a business card and urged him to get in touch with Adm. Michael Mullen, then chairman of the Joint Chiefs of Staff. Macedonia contacted Mullen and repeated his pitch. To his surprise, Mullen hired him.
At the time, “you had an entrenched military-medical community that did not want to go down that road,” Macedonia told me. “They didn’t want to give any credence to the idea that these symptoms were anything other than emotional difficulty.” Macedonia, an obstetrician as well as a soldier, knew otherwise. He did a tour in Anbar province in Iraq in 2004 and 2005 with soldiers who were being targeted frequently by mortars and roadside bombs. As an officer and doctor, he felt responsible for younger soldiers and their injuries. “Kids exposed to explosions were asking for help, and I was mouthing the party line: ‘You’ll be O.K.’ I was part of the machine that didn’t help. That’s what haunts me.”
Like Macedonia, some senior officers, including Gen. Peter Chiarelli of the Army and Gen. James Amos of the Marines, were also frustrated. They had seen too many soldiers discharged for disciplinary issues that were related to brain injury. Mullen hired several other experts to join Macedonia, asking them to monitor and improve the treatment of brain injury across the entire military. They called it the “Gray Team” — partly a play on gray matter and partly because the men were mostly in their 40s and going gray. They were an extraordinary group: mostly military officers, all of them had advanced degrees in medicine or science. And almost all of them had seen combat.
One of them was Jim Hancock, an emergency physician and Navy captain whose main qualification, he told me, was that he had suffered a traumatic brain injury himself, in southern Afghanistan. He also suffered concussions twice as a college athlete, so he had a basis for comparison. “The theory at the time was, it was a concussive event,” Hancock told me. “I said, ‘B.S.’ I’ve been concussed. I’ve never had anything like blast.” Like other members of the team, Hancock had noticed that soldiers exposed to blasts often had memory and focus problems that did not go away and that seemed distinct from battlefield trauma. If the blasts were repeated, the lapses sometimes devolved into career-ending mental and behavioral struggles. The Gray Team shared a gut-level belief that a blast wave’s effects on the body were far more extreme, and more complex, than the concussion model could account for. But their main task was to push the military to take brain injury more seriously, whatever its causes.
In early 2009, the Gray Team’s first five members traveled to military bases in Iraq and Afghanistan, meeting with trauma surgeons and other doctors to see how they handled brain injury. They found a wildly inconsistent picture. There were three extraordinary doctors who understood brain trauma and how to handle it. But “our fear was, those three rotate out, and it disappears,” said Dr. Geoffrey Ling, another member of the Gray Team.

Brandon Matthews, 33, is a former Army Ranger exposed to blasts in Iraq and elsewhere who now has cognitive problems. The 24 names tattooed on his back include war buddies who died in action or who killed themselves after coming home.
Nick Oza for The New York Times
When they got home, the team identified the most valuable practices and, along with Chiarelli and Amos, had them codified. Any soldier who was within 50 meters of a blast or who was in a vehicle behind or ahead of one struck by a bomb would have to be screened for brain injury. Anyone who suffered a concussion would have to be pulled out of combat. The Gray Team used a checklist to help identify concussed soldiers, although they were soon forced to write six different versions of it, because so many Marines memorized the correct answers to avoid being pulled out of combat. They also found a civilian contractor to build blast gauges, like the ones used in the breacher study. Every recruit or officer in a combat zone now wears three of these tiny devices, which weigh 20 grams each. The gauges are designed to turn red if they register a force of more than 12 pounds per square inch, the lower limit indicating a possible concussion or brain injury. The soldiers can no longer brush it off: If your sensor is red, you must be screened for brain injury.
The military has taken the new rules seriously. Less than a year after its first tour, the Gray Team went out to the field again and found that 90 percent of the bases they visited were in compliance. Still, the larger question of blast’s residue inside the skull remained a mystery.
Brandon Matthews is built like a tank, with huge humps of muscle outlining his back and shoulders. Ugly scars run down his biceps and forearms, cutting deep creases into the muscle. Others line his legs and sides, the legacy of an 11-year career as an Army Ranger. Matthews, registered with the military as Brandon Matthew Sipp, was exposed to so many blasts, in Iraq and other places, that he cannot count them all. The worst was a suicide bombing that sent him flying down a corridor and left him in a coma. He was hospitalized for months, and his military career was over. But his struggles with brain injury were only starting.
“I have moments when I forget everything: who I am, where I am, what I’m doing,” he told me. “It happens almost every day,” sometimes while he is driving. Decisions, once easy, have become impossible. He turns the kitchen burner on and then walks out, returning to discover a fire raging.
Matthews has 24 names tattooed down the center of his back. Eighteen are former war buddies who were killed in action. The more painful losses, in a sense, are five others: friends who have killed themselves since returning from the war. One of them, another Special Operations veteran with an undiagnosed traumatic brain injury, threatened his wife and children with a gun six months ago, Matthews told me, then shot himself in the head. Matthews spoke at the funeral. Undiagnosed blast injuries are common among the Special Operations soldiers, he said, because members of this military elite prize their toughness and do not want to risk losing their careers. “Here’s the harsh reality,” another veteran told me. “In the Special Forces especially, if I fail my physical, I’m done. That’s all there is to it. My cool-guy stuff is done.” So they keep their heads down, say nothing and suffer more blasts. Until one day, like Brandon Matthews, they are too damaged to fight.
I met Matthews at a hotel in Scottsdale, Ariz., where he now lives, and within an hour he had consumed several vodka-and-waters. He was warm and talkative, but every now and then he got a lost, plaintive look in his green eyes; I had the impression of a man who is clinging to a precipice. Before I could turn in, he insisted on steering me to a series of nightclubs, where he drank round after round and regaled strangers with his war stories. I asked him about friends, and he told me that almost all of them were dead. He lives on his military pension, and at 33, seems to have given up on holding down a job.
All this is fairly typical of service members and veterans who have suffered serious or repeated blast injuries, I was told by Susan Ullman, who runs an outreach network called Warrior2Warrior. (Ullman’s own husband, a Green Beret who suffered a traumatic brain injury, killed himself in 2013.) When I asked Matthews about other veterans and suicide, he grimaced and unleashed a string of obscenities about the cowardice of taking your own life. It felt cruel, and a little unnecessary, to ask if he had been tempted that way himself. (He has his own name tattooed on his back after those of friends who have killed themselves.)
Even if the underlying wounds of men like Matthews cannot be treated, the symptoms of brain injury, like those of trauma, can often be alleviated. The distinction between organic and emotional injury can be very blurry; trauma changes neuronal patterns, and therapy can alter a brain that has been physically damaged. “Everything we know suggests that people with structural lesion will also respond to pharmacological and psychological treatment,” said David Brody, a neurologist who has worked extensively with the military. Finding the right treatment is the key. Many veterans told me that they had gone to the V.A. and been handed pills indiscriminately. A number of mostly untested treatments have gained traction in the past few years, from hyperbaric chambers to ergonomic mouth guards, and some veterans swear by them.
For all his mental confusion, Matthews told me that he thinks he can now distinguish between the emotional wounds he suffered — the survivor’s guilt, the bad dreams and night terrors — and the more concrete cognitive problems that he traces to his blast exposure. A number of Special Operations soldiers said the same thing. They also said it makes a big difference to be told they have a physical wound rather than a mental one, even if it is incurable. Some brain injuries can now be seen on M.R.I.-type brain scans of living people, though precise diagnoses remain elusive. Matthews told me he would find some solace in simply being able to see what was going on inside his head.
Daniel Perl is continuing to examine the brains of blast-injured soldiers. After five years of working with the military, he feels sure, he told me, that many blast injuries have not been identified. “We could be talking many thousands,” he said. “And what scares me is that what we’re seeing now might just be the first round. If they survive the initial injuries, many of them may develop C.T.E. years or decades later.”
Perl takes some solace from the past. He has read a great deal about the men who suffered from shell shock during World War I and the doctors who struggled to treat them. He mentioned a monument in central England called “Shot at Dawn,” dedicated to British and Commonwealth soldiers who were executed by a firing squad after being convicted of cowardice or desertion. It is a stone figure of a blindfolded man in a military storm coat, his hands bound behind him. At his back is a field of thin stakes, each of them bearing a name, rank, age and date of execution. Some of these men, Perl believes, probably had traumatic brain injuries from blasts and should not have been held responsible for their actions. He has begun looking into the possibility of obtaining brain samples of shellshocked soldiers from that war. He hopes to examine them under the microscope, and perhaps, a century later, grant them and their descendants the diagnoses they deserve.
______________________________________
Robert F. Worth is a contributing writer for the magazine and the author of “A Rage for Order,” about the Arab Spring uprisings. He last wrote about Turkey’s hidden war against the Kurds.
DISCLAIMER: The statements, views and opinions expressed in pieces republished here are solely those of the authors and do not necessarily represent those of TMS. In accordance with title 17 U.S.C. section 107, this material is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. TMS has no affiliation whatsoever with the originator of this article nor is TMS endorsed or sponsored by the originator. “GO TO ORIGINAL” links are provided as a convenience to our readers and allow for verification of authenticity. However, as originating pages are often updated by their originating host sites, the versions posted may not match the versions our readers view when clicking the “GO TO ORIGINAL” links. This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more information go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.