
Facts about Covid-19
COVID19 - CORONAVIRUS, 28 Sep 2020
Swiss Policy Research - TRANSCEND Media Service
Sep 2020 – Fully referenced facts about Covid-19, provided by experts in the field, to help our readers make a realistic risk assessment. (Regular updates below)
“The only means to fight the plague is honesty.” (Albert Camus, 1947)
Overview
- According to the latest immunological studies, the overall lethality of Covid-19 (IFR) in the general population ranges between 0.1% and 0.5% in most countries, which is comparable to the medium influenza pandemics of 1957 and 1968.
- For people at high risk or high exposure (including health care workers), early or prophylactic treatment is essential to prevent progression of the disease.
- In countries like the UK (with lockdown) and Sweden (without lockdown), overall mortality since the beginning of the year is in the range of a strong influenza season; mortality is higher in the USA (comparable to 1957/1968), but lower in countries like Germany and Switzerland. However, antibody values are still low in large parts of previously locked-down Europe.
- In most places, the risk of death for the healthy general population of school and working age is comparable to a daily car ride to work. The risk was initially overestimated because many people with only mild or no symptoms were not taken into account.
- About 80% of all people develop only mild symptoms or no symptoms. Even among 70-79 year olds, about 60% develop only mild symptoms. About 95% of all people develop at most moderate symptoms and do not require hospitalization.
- Up to 60% of all people may already have a partial T-cell immune response against the new coronavirus due to contact with previous coronaviruses (i.e. cold viruses). Moreover, up to 60% of children and about 6% of adults may already have cross-reactive antibodies.
- The median age of Covid deaths in most Western countries is over 80 years – e.g. 84 years in Sweden – and only about 4% of the deceased had no serious preconditions. In contrast to flu pandemics, the age and risk profile of deaths thus essentially corresponds to normal mortality.
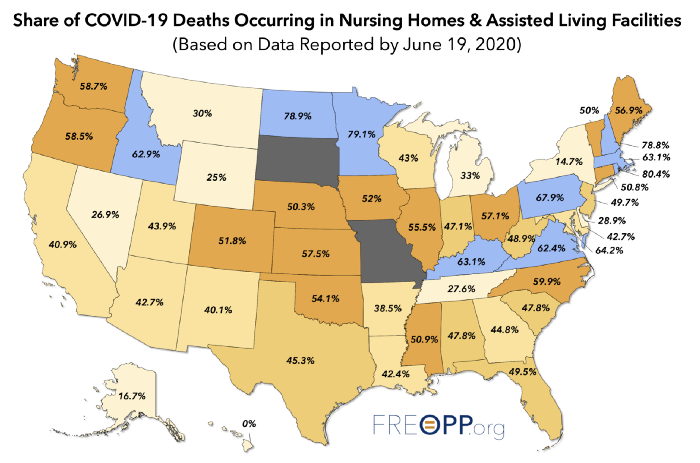
- In many countries, up to two thirds of all extra deaths occurred in nursing homes, which do not benefit from a general lockdown. Moreover, in many cases it is not clear whether these people really died from Covid-19 or from weeks of extreme stress and isolation.
- Up to 30% of all additional deaths may have been caused not by Covid-19, but by the effects of the lockdown, panic and fear. For example, the treatment of heart attacks and strokes decreased by up to 40% because many patients no longer dared to go to hospital.
- Many media reports of young and healthy people dying from Covid-19 turned out to be false: many of these young people either did not die from Covid-19, they had already been seriously ill (e.g. from undiagnosed leukaemia), or they were in fact 109 instead of 9 years old. The claimed increase in Kawasaki disease in children also turned out to be exaggerated.
- Most Covid-19 symptoms can also be caused by severe influenza (including pneumonia, thrombosis and the temporary loss of the sense of taste and smell), but with severe Covid-19 these symptoms are indeed much more frequent and more pronounced.
- About 10% of symptomatic people develop so-called post-acute (“long”) Covid and report symptoms that last for several weeks or months. This may also affect younger and previously healthy people with a strong immune response to the new coronavirus.
- The often shown exponential curves of “corona cases” are misleading, as the number of tests also increased exponentially. In most countries, the ratio of positive tests to tests overall (i.e. the positivity rate) always remained below 20%. In many countries, the peak of the spread was already reached well before the lockdown came into effect.
- In most Covid hotspots, including New York City, London, Stockholm and Bergamo, the infection rate dropped as soon as about 20% of people had developed antibodies against the new coronavirus. This value is much lower than the inital estimate of 60 to 80%.
- Countries without lockdown, such as Japan, Belarus and Sweden, have not experienced a more negative course of events than many other countries. Sweden was even praised by the WHO and now benefits from higher immunity compared to lockdown countries. 75% of Swedish deaths happened in nursing facilities that weren’t protected fast enough.
- The fear of a shortage of ventilators was unjustified. According to lung specialists, the invasive ventilation (intubation) of Covid-19 patients, which is partly done out of fear of spreading the virus, is in fact often counterproductive and damaging to the lungs.
- The main routes of transmission of the virus are direct contact and droplets produced when talking or coughing, but also indoor aerosols (small particles floating in the air). Outdoor aerosols and surfaces of objects appear to play only a minor role.
- There is still little to no scientific evidence for the effectiveness of cloth face masks in the general population, and the introduction of mandatory masks couldn’t contain or slow the epidemic in most countries. Some experts warn that face masks may interfere with normal breathing and may become “germ carriers” if used repeatedly.
- Many clinics in Europe and the US remained largely underutilized during lockdowns and in some cases had to send staff home. Millions of surgeries and therapies were cancelled, including many cancer screenings and organ transplants.
- Several media were caught trying to dramatize the situation in hospitals, sometimes even with manipulative images and videos. In general, the unprofessional reporting of many media maximized fear and panic in the population. As a result, according to international surveys, most people dramatically overestimate Covid-19 lethality and mortality.
- The virus test kits used internationally may in some cases produce false positive and false negative results, react to non-infectious virus fragments from a previous infection, or react to other common coronaviruses with a partially similar gene sequence.
- Numerous internationally renowned experts in the fields of virology, immunology and epidemiology consider the measures taken to be counterproductive and recommend rapid natural immunization of the general population and protection of risk groups.
- At no time was there a medical reason for the closure of elementary schools, as the risk of disease and transmission in children is extremely low. There is also no medical reason for small classes, masks or ‘social distancing’ rules in elementary schools.
- Several medical experts described express coronavirus vaccines as unnecessary or even dangerous. Indeed, the vaccine against the so-called swine flu of 2009, for example, led to cases of severe neurological damage and lawsuits in the millions. In the testing of new coronavirus vaccines, too, serious complications and failures have already been reported.
- A global respiratory disease pandemic can indeed extend over several seasons, but many studies of a “second wave” are based on very unrealistic assumptions, such as a constant risk of illness and death across all age groups.
- US nurses described an oftentimes fatal medical mismanagement of Covid patients due to questionable financial incentives and inappropriate medical protocols. However, in many places Covid lethality has dropped significantly due to better treatment options.
- The number of people suffering from unemployment, depression and domestic violence as a result of the measures has reached historic record levels. Several experts predict that the measures will claim far more lives than the virus itself. According to the UN 1.6 billion people around the world are at immediate risk of losing their livelihood.
- NSA whistleblower Edward Snowden warned that the “corona crisis” may be used for the permanent expansion of global surveillance. In several parts of the world, the population is being monitored by drones and facing serious police overreach during lockdowns.
- A 2019 WHO study on measures against pandemic influenza found that from a medical perspective, “contact tracing” is “not recommended in any circumstances”. Nevertheless, contact tracing apps have already become partially mandatory in several countries.
- The origin of the new coronavirus remains unknown, but the best evidence currently points to a Covid-like pneumonia incident in a Chinese mine in 2012, the viral samples of which were collected, stored and examined by the Wuhan Institute of Virology (WIV).
Read more: On the treatment of Covid-19
Bill Gates on vaccine side effects (CBS, July 23, 2020)
See also
- On the treatment of Covid-19
- Studies on Covid-19 lethality
- The evidence on face masks
- On post-acute (“long”) Covid
- On the origin of SARS-CoV-2
Overview diagrams






September 2020
Medical updates
- Covid lethality: Most Western countries report a covid lethality (IFR) of about 0.3% in the general population (excluding nursing homes). The IFR may be even lower as antibody tests appear to miss about half of all infections. The IFR is higher if there was a local collapse of health care or elderly care. Countries with a younger population report lower IFRs: India reports about 0.1%, African countries report about 0.01%. Read more.
- Why covid is a “strange pandemic”: Why does covid-19 appear to be a somewhat strange pandemic? It is because of the covid-19 mortality profile, which is almost identical to natural mortality. But this doesn’t mean covid is just a “casedemic”. Read more.
- Face masks: Evidence from around the world indicates that cloth face masks used by the general population have little to no impact on coronavirus infection rates. The WHO study on face masks and social distancing turned out to be seriously flawed.
- Treatment of covid-19: Early or prophylactic treatment of covid-19 is essential to prevent progression of the disease. New studies confirm the effectiveness of zinc, vitamin D, bromhexine and malaria drug HCQ in early treatment of high-risk patients. Read more.
- Disease mechanisms: Several new studies show that (severe) covid is first and foremost a cardiovascular disease that causes thrombosis (blood clotting) and lung embolism by damaging the blood vessels. This explains the age and risk profile of covid-19 mortality.
- Post-acute (“long”) covid: About 10% of symptomatic people, including young and healthy people, develop “long covid” that may last for several weeks or months. Of particular concern is the impact of the new coronavirus on the heart muscle. Read more.
- PCR tests: As previously reported, many of the people testing positive may not carry infectious virus. A new analysis now confirms that in the US, up to 90% of positive PCR tests may have been “false positives” detecting non-infectious virus fragments.
- Origin of the new coronavirus: Evidence is increasing that the new coronavirus may be linked to a covid-like pneumonia incident in a Chinese mine back in 2012. Read more.
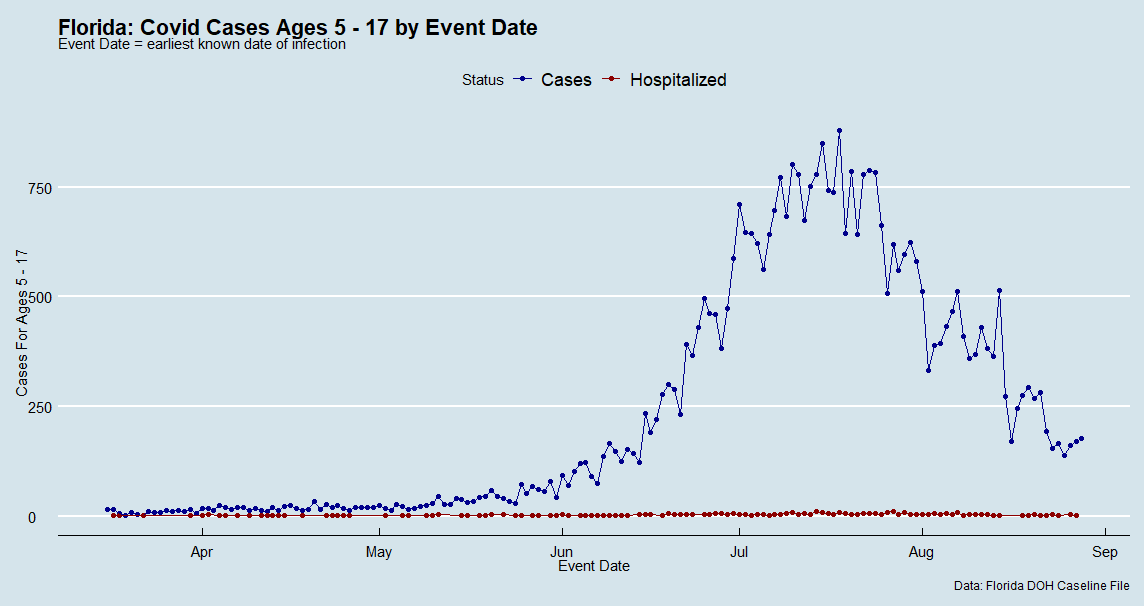
- Children: The risk of transmission and disease in children continues to be extremely low. The following chart shows cases and hospitalizations of children in Florida.
Country profiles
In large parts of previously locked-down Europe as well as in parts of the US, antibody values are still rather low and the risk of a renewed increase in coronavirus infections and disease is therefore high. Read our latest covid-19 country profiles:
- USA: Several short regional waves, mortality comparable to 1957/68 flu pandemics
- Germany: No excess mortality so far, but still very low antibody values
- Sweden: No lockdown, no masks, mortality comparable to strong flu wave.
- Australia and New Zealand: Last Western countries following a zero-covid strategy
- Africa and Latin America: Lowest and highest covid mortality in the world.
- Belarus: Very low covid mortality despite no lockdown; unique demographics.
- Belgium: Very high mortality; 66% of deaths occurred in nursing homes.
- Italy: Huge differences between northern and southern Italy.
- Nembro (Italy): The hardest hit place in Europe. What happened?
- Switzerland: Low mortality in spring, but very low antibody values.
Political updates
- IMF, World Bank: Covid lockdowns and economic recession may drag 100 million people into extreme poverty and set back poor nations by ten years.
- Professor Mark Woolhouse (UK): Lockdown will come to be seen as a “monumental mistake on a global scale” and must never happen again. The equivalent of 400 million jobs have been lost world-wide, 13 million in the U.S. alone.
- Australia: Extreme lockdown in Melbourne (Victoria) – more suicides than covid deaths.
- Germany: German police may have staged a run on the federal parliament in order to discredit a peaceful protest by about 100,000 people against political corona measures.
- Contact tracing: Back in May, Google and Apple implemented a “contact tracing” interface into three billion mobile phones. In early September, they integrated it even deeper into their operating systems, enabling contact tracing without an official app and on a global scale. From a medical perspective, there is still no evidence that “contact tracing” reduces the covid infection rate. Swiss IT professor Serge Vaudenay warned that the Google-Apple interface is not transparent and may record every single contact.
- Vaccines: Covid vaccine manufacturers have received a liability waiver in most countries. The Oxford vaccine trial has been suspended after a serious neurological adverse event occurred. A Belgian journalist moreover reported temporary fever, severe chest pain, “glowing hot legs” and loss of all feeling in his fingers after receiving another covid vaccine.

Additional resources
For daily covid updates from an independent perspective, see also Lockdown Skeptics (UK), CovidInfos (France), and Corona Transition (Switzerland/Germany/Austria).
August 2020
A. General part
Pre-existing immunity against the new coronavirus
At the beginning of the Covid-19 pandemic, it was assumed that no immunity against the new coronavirus existed in the population. This was one of the main reasons behind the initial strategy of “flattening the curve” by introducing stay-at-home orders.
From March and April onwards, however, the first studies showed that a considerable part of the population already had a certain background immunity to the new virus, acquired through contact with earlier coronaviruses (common cold viruses). Nevertheless, it remains unclear to what extent this “background immunity” may indeed protect against the new coronavirus.
Further important studies on this topic were published in July:
- A new study from Germany came to the conclusion that up to 81% of people who have not yet had contact with the new coronavirus already have cross-reactive T-cells and thus a certain background immunity. This confirms earlier studies on T-cell immunity.
- In addition, a British study found that up to 60% of children and adolescents and about 6% of adults already have cross-reactive antibodies against the new coronavirus, which were created by contact with previous coronaviruses. This is probably another important aspect in explaining the very low rate of disease in children and adolescents.
- In the case of Singapore, a study published in the scientific journal Nature concluded that people who contracted SARS-1 in 2002/2003 still had T-cells that were reactive against the new SARS-2 coronavirus 17 years later. In addition, the researchers found cross-reactive T-cells, which were produced by contact with other, partly unknown coronaviruses, in about half of the people who had neither contracted SARS-1 nor SARS-2. The researchers suspect that the different distribution of such coronaviruses and T-cells may help explain why some countries are less affected than others by the new corona virus, regardless of the political and medical measures taken.
- Analysts have previously pointed out that many Pacific countries, and especially China’s neighbouring countries, have so far had very low Covid death rates, regardless of their population structure (young or old) and the measures taken (with or without lockdown, mass tests, masks, etc.). A possible explanation for this could be the spread of earlier coronaviruses.
- Harvard immunologist Michael Mina explained that the “drop in antibody concentration” after Covid disease, dramatized by some media, was “perfectly normal” and “textbook”. The body ensures long-term immunity through T-cells and memory cells in the bone marrow, which can quickly produce new antibodies when needed.
See also: Immunological studies on the new coronavirus
Other medical updates
Wuhan: A Harvard modelling study in the scientific journal Nature came to the conclusion that even in the Covid epicentre Wuhan, up to 87% of the infections went unnoticed, i.e. remained without symptoms or mild. This means that the Covid19 lethality (IFR) in Wuhan may also fall to about 0.1% or below. The Nature study confirms an earlier Japanese study in the journal BMC Medicine, which calculated an IFR of 0.12% for Wuhan already back in March.
However, Chinese authorities couldn’t yet know this comparatively low lethality in January and February and therefore built additional clinics at short notice, many of which eventually remained mostly unused. Only the systematic test results from South Korea and the cruise ship Diamond Princess showed that the lethality of the new corona virus in the general population is indeed lower than initially feared.
Italy: The Italian health authority ISS published a new analysis of the cause of death in about 5000 corona patients. According to this analysis, Covid was the direct cause of death in 89% of the cases. In 11%, other diseases such as heart problems, cancer or dementia were the primary cause of death. Covid was the sole cause of death in 28% of cases. It is also known that in about 4% of the deaths, no medical preconditions were present.
Covid lethality: In May, the US health authority CDC published a cautious “best estimate” of covid lethality (IFR) of 0.26% (assuming 35% asymptomatic infections). In July, a new IFR of 0.65% was published. However, this new value is not based on own calculations or new studies, but on a meta-study in which the existing literature was simply searched for all previous IFR values.
Thus, the meta-study mainly consists of previous modelling studies as well as “raw IFR values”, which are much too high compared to the actual, population-based IFR values from antibody studies. With few exceptions, the real IFR values are between 0.1% and 0.4%, and when mucosal and cellular immunity are taken into account, they are approximately 0.1% or less.
However, the virus has spread much faster than anticipated, thus causing a temporarily high death rate in some places, especially if nursing homes and hospitals got affected.
Non-infectious virus fragments: The U.S. CDC points out that in most Covid patients, infectious virus particles are no longer detectable ten to fifteen days after the first symptoms. However, non-infectious virus fragments (RNA) can still be found up to three months after the first symptoms. This is likely to be a significant problem with regard to PCR tests, as many people who have long since ceased to be infectious still test positive, triggering far-reaching tracing and quarantine false-alarms.
Deaths with or by or without coronavirus: In England and some other countries it has been reported that all deceased persons who tested positive for the new coronavirus since the beginning of the year were counted as Covid deaths – regardless of the time of the test, a possible recovery, and the actual cause of death. In the US state of Colorado, it was found that about 10% of deaths were with but not from coronavirus. In other US states, further cases of “corona deaths” became known that in reality were test-positive homicide victims and motorcycle accidents.
Children and schools
It has been known since March that the risk of disease and transmission in children is minimal in the case of Covid19. The main reason for this is probably a pre-existing immunity due to frequent contact with previous coronaviruses (i.e. cold viruses). There was and is therefore no medical reason for the closure of primary schools, kindergartens and day-care centres and for special protective measures in schools.
In the meantime, further studies on this issue have been published:
- The British epidemiologist Professor Mark Woolhouse stated that there is not a single confirmed case of infection of a teacher by a pupil worldwide.
- Tracing pioneer Iceland found “not a single case where a child under 10 infected their parents.”
- US CDC director Robert Redfield explained that additional deaths from suicides and drug overdoses by adolescents have been “far greater” than Covid deaths in recent months.
- A joint report from Sweden (without primary school closure) and Finland (with primary school closure) concluded that there was no difference in infection rates among children in the two countries.
- In the USA, three times more children up to 14 years of age have died of influenza than of Covid-19 (101 versus 31) since the beginning of the year, according to the CDC.
- A Canadian study found that most of the children with “Kawasaki-like” inflammatory symptoms had no corona infection at all. The disease in children is “very, very rare”, the researchers said.
- A German study came to the conclusion that children act epidemiologically “like brake blocks” and slow down the spread of the new corona virus.
Critical expert opinions
- The German virologist Hendrik Streeck advocates a pragmatic approach to the new coronavirus and targeted measures for people at high risk. According to Streeck, the long-term suppression of the virus and the hope for a possible vaccine are not sensible strategies.
- Professor Carl Heneghan, Director of the Oxford Centre for Evidence-Based Medicine, explains in an interview that there is still no evidence for the effectiveness of masks in the general population. A permanent suppression strategy like the one in New Zealand is not sensible and causes high damage in the long term. The lethality (IFR) of Covid-19 is about 0.1% to 0.3% and is thus comparable to previous flu epidemics and pandemics.
- The Swedish chief epidemiologist Anders Tegnell explains in an interview that eradication of the virus is not an option. In Sweden, the infections slowed down considerably even without a lockdown, and daily deaths now are close to zero. The evidence for the benefit of masks is still “very weak” and they might even be counterproductive. An introduction of masks at this point in time would make no sense. The lethality of Covid-19 is between 0.1% and 0.5% and does not “radically differ” from influenza.
- The epidemiologist and systems biologist Professor Francois Balloux, Director of the British UCL Genetics Institute, explains in an article that Covid-19 is comparable to a pandemic (but not seasonal) influenza. The main difference is the age-risk distribution: while Covid-19 is mainly dangerous for older people, a pandemic influenza is also life-threatening for younger people and children. Professor Balloux points out that the “Russian influenza pandemic” of 1889 may have been triggered by the coronavirus OC-43, which is now considered one of the four typical cold viruses.
- The Swiss chief physician for infectiology, Dr. Pietro Vernazza, pleads for a “controlled natural immunization” of society as an alternative to the “eradication strategy”. In most cases, Covid-19 is mild and the actual mortality rate is about 0.1%, which is in the range of a severe influenza. The Swedes “did nothing wrong” with their strategy, according to Vernazza.
- The former director of the Institute of Immunology at the University of Bern, Professor Beda Stadler, also pleads for a controlled spread of the virus. The danger of the virus had been overestimated due to the false assumption of a lack of immunity. Professor Stadler is critical of compulsory masks and mass tests. Stadler, who is now emeritus, explains that many younger immunologists no longer dare to speak out publicly on the subject due to the extreme polarisation of the debate by politics and the media.
On the other hand, Professor Karin Mölling, the former head of the Department of Virology at the University of Zurich and one of the earliest critical voices on corona measures, has now partly changed her opinion: Due to the sometimes serious lung damage, the virus should not be underestimated and containment measures are important.
The clinical picture of Covid-19
The lower-than-expected lethality of Covid-19 should not hide the fact that the new coronavirus, due to its efficient use of the human ACE2 cell receptor, in some cases can lead to severe disease with complications in the lung, the vascular and nervous systems and other organs, some of which can persist for months.
While it is true that most of these symptoms can also occur in severe influenza (including thrombosis, heart muscle inflammation, and the temporary loss of the sense of smell), they are indeed more frequent and more pronounced in the novel Covid-19 disease.
In addition, even apparently “mild” disease (without hospitalization) can in some cases lead to protracted complications with breathing problems, fatigue or other symptoms. The US CDC came to the conclusion that after one month, about one third of the “mild” cases still showed such symptoms. Even in the 18 to 34-year-olds without preconditions, about 20% still had after-effects.
On the positive side, researchers at a German clinic recently reported good chances of recovery: “We can see that the lungs can heal well, even in patients who have had three weeks of intensive care”. After three months, 20% of the intensive care patients had healthy lungs again, and in the remaining patients a clear regeneration was visible.
Nevertheless, the primary goal should be to avoid a progression of the disease.
On the treatment of Covid-19
Note: Patients are asked to consult a doctor.
Many countries adopted the strategy of imposing a lockdown during or after a wave of infection, thereby locking already infected high-risk individuals in their homes without treatment until they developed severe breathing problems and needed intensive care treatment immediately. Even today, test-positive high-risk persons are often simply quarantined without treatment.
This is not an ideal approach. Numerous studies and doctors’ reports have now shown that for people at high risk or with high exposure, early treatment immediately on onset of the first typical symptoms is crucial to avoid disease progression and hospitalization.
Studies and medical reports from various countries in Asia and the West recommend a combination protocol of zinc (which inhibits the RNA replication of coronaviruses), the antimalarial agent HCQ (which promotes the cellular uptake of zinc and has other anti-viral properties), and, if necessary, an antibiotic (to prevent bacterial superinfections) and a blood thinner (to prevent thrombosis and lung embolism).
Yale professor and physician Harvey A. Risch argues in a recent commentary that early treatment with HCQ and zinc as well as an antibiotic has proven to be “highly effective”. In the USA alone, according to Professor Risch, 70,000 to 100,000 deaths could have been prevented by the systematic use of HCQ. Risch is therefore calling for an immediate and prescription-free release of this medication, as is already the case in many other countries.
Meanwhile, a bizarre battle has broken out in western industrialised countries over the use of low-cost HCQ, which has been used successfully and safely for decades in the prevention and treatment of malaria and several other diseases. This battle appears to be driven in part by political and commercial interests and may produce a great many casualties.
Opponents of HCQ went as far as publishing falsified studies and using lethal doses during trials, as Dr. James Todaro explains, who uncovered one of these frauds that fooled top science journals, the WHO and health experts worldwide.
Many of these anti-HCQ activities are connected to pharmaceutical company Gilead, which wants to sell a drug that is over a hundred times more expensive (Remdesivir), but which is only used on intensive care patients and has some severe side effects.
In addition, a potentially effective early treatment stands in the way of the billion-dollar global vaccination strategy being pursued by numerous governments, pharmaceutical companies and vaccine investor Bill Gates. Directors of vaccine companies have already made about one billion dollars with stock and option gains alone, even without yet delivering a vaccine.
The hope for a safe and effective vaccine, however, remains questionable: Contrary to the positive media presentation, in the second test round of the RNA vaccine from the US company Moderna, 80% of the volunteers in the medium and high-dose groups (average age 33 years and healthy) reacted with moderate to severe side effects.
The effectiveness of face masks
Various countries are discussing or have already introduced mandatory face masks in the general population. In the updates of June and July, however, it was shown that the evidence for the effectiveness of cloth masks in the general population is still rather weak, contrary to what is reported in many media.
In previous influenza pandemics, cloth masks had no influence on the occurrence of infection. Despite masks, Japan had its last flu epidemic with more than five million diseased just one year ago, in January and February 2019. Even the outbreak of the Covid pandemic in Wuhan could not be stopped by the widespread use of masks there.
Due to the significantly lower hospitalisation and mortality rates of Covid-19 (compared to the original assumptions), masks are not necessarily required to “flatten the curve”. Masking only makes sense – if at all – in the context of a vaccination strategy that aims to suppress the virus until a vaccine is available.
BBC medical correspondent Deborah Cohen explained in mid-July that the partial update of the WHO recommendation on masks was due not to new evidence but “political lobbying”: “We had been told by various sources WHO committee reviewing the evidence had not backed masks but they recommended them due to political lobbying. This point was put to WHO who did not deny.”
The “political lobbying” is likely referring to the group “Masks for All”, which was founded by a “Young Leader” of the Davos forum and which is lobbying authorities and governments for a worldwide face mask obligation.
In connection with masks, the question also arises as to whether the new coronavirus can be transmitted over large areas by aerosols. According to experts, true aerosol transmission even outdoors still seems unlikely – otherwise the spread of the virus would have a different dynamic and, contrary to reality, would often be untraceable.
However, an aerosol-like transmission indoors – especially with closed air circulation by fans or during intensive activities such as singing and dancing – seems increasingly probable or certain due to various incidents.
In the case of aerosol transmission, however, cloth masks are likely to offer even less protection than against droplets due to their pore size and inaccurate fit. This was demonstrated, for example, by the corona outbreak at the German meat processor Toennies, which occurred at an air-conditioned workplace over a distance of up to eight metres despite the requirement to wear masks.
On the question of “asymptomatic transmission”, it can currently be said that true asymptomatic transmission still seems to be rare (which may explain the very low transmission rate in children), whereas pre-symptomatic transmission in the days before the first symptoms appear (with already high virus load) is very likely and may explain the rapid spread of the virus.
Pre-symptomatic transmission is also known from influenza, but the incubation period of influenza is much shorter, so this may be somewhat less relevant.
The following expert reviews and articles critically examine the effectiveness of cloth masks in the general population:
- Profs. Tom Jefferson and Carl Heneghan (Oxford): Masking lack of evidence with politics
- Dr. Lisa Brosseau and Dr. Margaret Sietsema, Center for Infectious Disease Research and Policy, University of Minnesota: Masks-for-all for COVID-19 not based on sound data
- Professor Michael T. Osterholm, Center for Infectious Disease Research and Policy, University of Minnesota: My views on cloth face coverings for the public for preventing COVID-19
- Naoya Kon: Cloth face masks offer zero shield against virus, a study shows
- Eliza McGraw: Everyone wore masks during the 1918 flu pandemic. They were useless.
The Swedish chief epidemiologist Anders Tegnell recently stated that the introduction of masks at this point in time, and even in public transport, would be “pointless” in view of the rapidly decreasing number of cases in Sweden. The Dutch government has stated that it will not in general recommend masks because the scientific evidence for their effectiveness is weak.
On the other hand, face masks are not harmless, as the following evidence shows:
- The WHO warns of various “side effects” such as difficulty breathing and skin rashes.
- Tests conducted by the University Hospital of Leipzig have shown that face masks significantly reduce the resilience and performance of healthy persons.
- A German psychological study with about 1000 participants found “severe psychosocial consequences” due to the introduction of mandatory face masks in Germany.
- The Hamburg Environmental Institute warned against the inhalation of chlorine compounds in polyester masks as well as problems in connection with disposal.
- The European rapid alert system RAPEX has already recalled 70 mask models because they did not meet EU quality standards and could lead to “serious risks”.
- In China, two boys who had to wear a mask during sports classes fainted and died.
- In the US, a car driver wearing an N95 (FFP2) mask fainted and crashed into a pole.
Conclusion: It is still possible that cloth masks can slow down the rate of infection in the general population, but the evidence for this is currently limited and the potential benefits are mainly relevant in the context of a long-term and still uncertain vaccination strategy.
Read more: Are face masks effective? The evidence.
Is Covid-19 a pure “test epidemic”? Certainly not.
Some particularly skeptical observers still seem to perceive Covid-19 mainly or solely as a “test epidemic”. However, this position has been untenable for months already.
The best known “test epidemic” is the so-called swine flu of 2009/2010, a rather mild influenza virus that only caused worldwide anxiety due to mass testing and media panic. A commission of the Council of Europe later called the swine flu a “fake pandemic” and a “big pharma fraud”.
What was noteworthy at the time was that a few months earlier, the WHO changed its pandemic guidelines and removed the criterion of increased lethality. In addition, pharmaceutical companies signed secret contracts worth billions with governments for a vaccine that later led to sometimes serious neurological damage and had to be disposed of for the most part.
Finally, researchers discovered that the swine flu virus itself probably originated from vaccine research and was released through a leak (or worse).
On the other hand, due to its special characteristics – in particular the very efficient use of the ACE2 cell receptor – the new coronavirus is a rather dangerous and easily transmissible SARS virus which can cause severe damage to the lungs, blood vessels and other organs. The good fortune is that many people already have a certain immunity to the new virus or at least are able to neutralize it on the mucosal membrane.
Covid-19 is therefore a real and serious pandemic and comparable to the (still stronger) flu pandemics of 1957/58 (Asian flu) and 1968 to 1970 (Hong Kong flu). The comparison with the swine flu of 2009 is only possible because the deaths caused by swine flu were greatly exaggerated.
(On the other hand, it should be remembered that during the 1968/1970 flu pandemic – or rather in the summer between the two main waves – the famous Woodstock festival was held and social life mostly went on as usual).
However, it can be argued that the real Covid19 pandemic has been amplified by a “test pandemic” due to mass testing in the general population, causing additional panic and high costs.
Stanford Professor Scott Atlas argued already in May that mass testing in the general population is of little use and that testing should instead be limited to vulnerable institutions such as nursing homes and hospitals (including for visitors).
Daily mass testing is also not effective because, according to antibody studies, the virus is already much more widespread than PCR tests show, anyway. Moreover, the tests are susceptible to false-positive (and false-negative) results and non-infectious virus fragments.
Countries such as Japan, Sweden and Belarus have shown that the pandemic can be controlled without a lockdown and without mass testing – and in the case of Sweden and Belarus also without masks – as long as the sensitive facilities are protected.
Conclusion: Covid-19 is a real and serious pandemic comparable to the (still stronger) influenza pandemics of 1957 and 1968, but in addition to the real Covid-19 pandemic, there is indeed a “test pandemic” that causes unnecessary panic and high costs.
The origin of the new coronavirus
The origin of the new SARS coronavirus remains unclear. However, researchers with access to Chinese documents were able to show in May that the closest related coronavirus was found in a mine in southwest China, where six miners contracted Covid-like pneumonia in 2012 and three of them died.
The miners’ illness was clinically virtually identical to today’s (severe) Covid-19, which is why some analysts have proposed to call the disease Covid-12 instead of Covid-19.
The Virological Institute in Wuhan received virus samples from the mine as well as from the tissue of the deceased miners in 2012 and 2013. It is conceivable that this virus escaped from the laboratory in autumn 2019.
In addition to the Chinese institute, however, the US health authority CDC and the US Department of Defense have also been shown to be working with SARS-like viruses from bats. The US NGO “Eco Health Alliance” cooperated on this issue with both the US Pentagon and the Virological Institute in Wuhan.
Direct transmission by an animal is also still conceivable, although previous candidates such as the well-known animal market in Wuhan or the Pangolin theory have been ruled out by experts in the meantime.
Read more: Origin of Covid-19 Virus: The Mojiang Miner Hypothesis
B. Countries and regions
USA
The USA is one of the countries most affected by the new coronavirus so far. This could have political and medical reasons.
Medically, there are many relevant pre-existing conditions in the US population, such as obesity, heart problems and diabetes. Air conditioning systems could promote aerosol-like transmission indoors. Politically, there have been serious mistakes in dealing with nursing homes, misplaced incentives in the treatment of patients, and problematic back-and-forth with lockdowns.
- The US already has over 150,000 corona deaths, putting it in the range of a pandemic influenza, comparable to the 1957 and 1968 pandemics.
- 45% of corona deaths occurred in nursing homes. Over 50% of all deaths occurred in the six states that actively placed Covid patients in nursing homes.
- For people of school and work age (up to 65), corona mortality is comparable to mortality from other pneumonia diseases (e.g. influenza), according to the CDC. For children and adolescents, Covid is three times less dangerous than influenza.
- A nationwide antibody study showed that the new coronavirus is 6 to 24 times more widespread than assumed on the basis of PCR tests, depending on the region. However, the antibody levels are still in the single-digit percentage range in most regions, indicating that exposure to the coronavirus is less much less than 50% in many places.
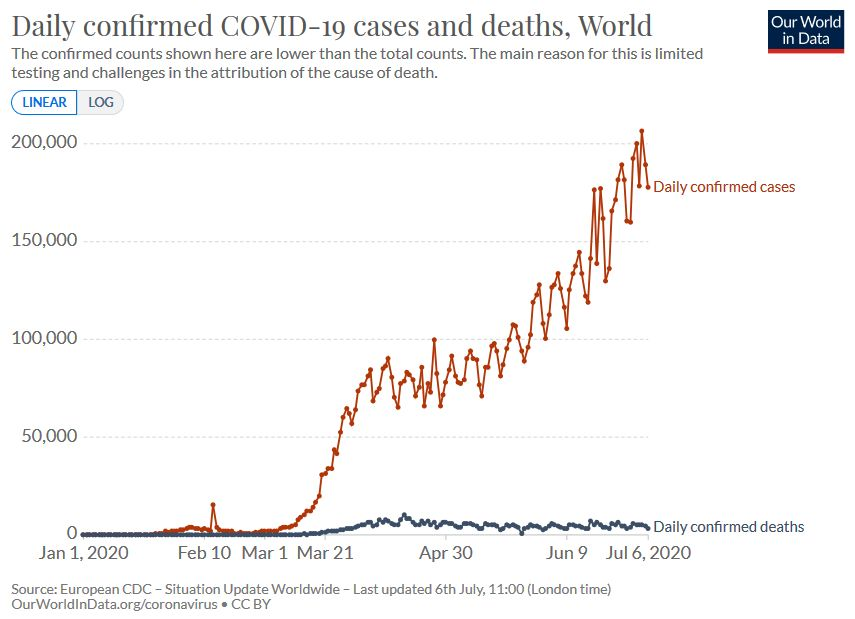
- While the number of daily positive tests reached a peak in mid-July due to the high number of tests, the number of daily deaths was only half as high as in April, although recently with a slight upward trend again (see graph below).
- In Florida there were reports of at times allegedly very high positivity rates. However, an analysis showed that various laboratories only reported the number of positive tests and thus an apparent positivity rate of 100%. The actual positivity rate in Florida was mostly in the single-digit percentage range. In terms of deaths per capita, Florida remains in the lower midfield compared to the other states.
- The median age of Covid deaths in the USA is 78.5 years. This is higher than the median age of “other deaths”, but lower than the median age of Covid deaths in Europe (80 to 86).
- Yale professor and epidemiologist Harvey A. Risch recently called for immediate over-the-counter availability of HCQ for the early treatment of Covid disease.
- A group of doctors calling itself “America’s Frontline Doctors” held a press conference with the same goal of making HCQ available. The video of the press conference was seen by 20 million people within a day before it was deleted by Facebook & Co. as “misinformation”.

Great Britain
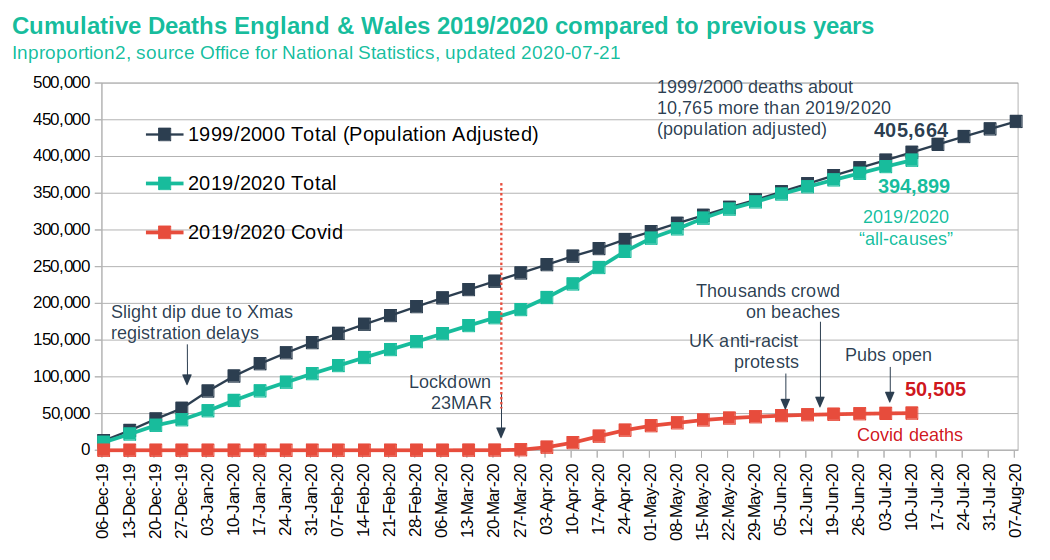
- In England and Wales there have been about 50,000 corona deaths so far. The overall mortality rate is thus still about 10,000 deaths below the strong flu epidemic of 1999/2000.
- There has been no excess mortality among those under 45 years of age compared to the last five years.
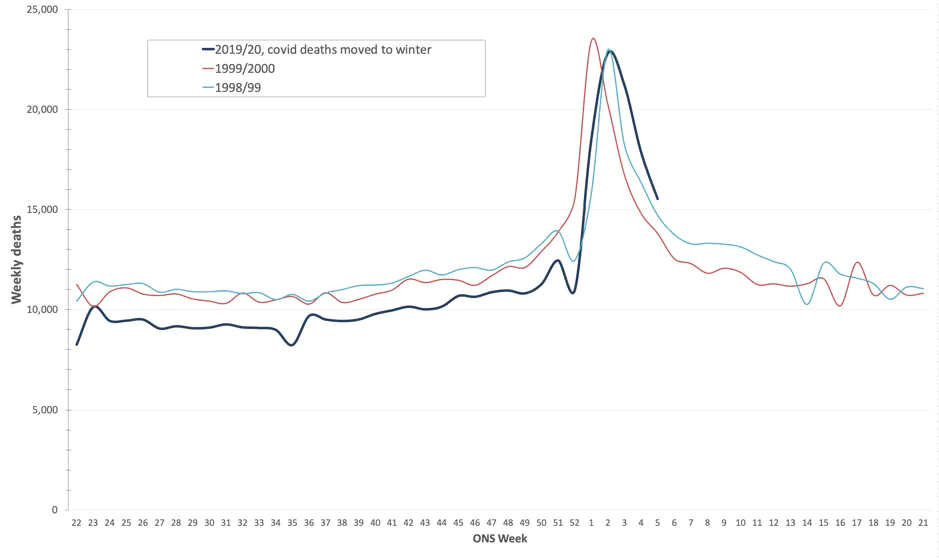
- The cumulative corona deaths since March correspond almost exactly to the cumulative influenza and pneumonia deaths since the start of the winter season in December 2019.
- Since mid-June, England and Wales have been in relative under-mortality and daily corona deaths have been below daily influenza and pneumonia deaths since then.
- By mid-April, 45% of NHS nursing staff had already been infected with corona. A significant proportion of patients may have been infected with corona in hospital. Corona patients were also transferred to nursing homes in England, which led to additional deaths.
France
France was relatively hard hit by the corona pandemic and registered about 30,000 corona deaths by the end of May according to the health authority SPF. About 50% of these deaths occurred in nursing homes, the average age of the deaths is 81.3 years. The median age of intensive care patients was about 67 years.
The region around Paris, eastern France and northern France were particularly hard hit, while large parts of western France and southwestern France were hardly affected at all (so far).
So although only part of France was affected by Covid, the cumulative excess mortality since the beginning of the year (compared to the baseline) is about 50% higher than during the seasonal flu waves of the past five years. In Greater Paris, the excess mortality rate is even around 500% or 10,000 people higher than in previous years (see graphs below).
Covid deaths accounted for around 16% of all deaths nationwide, but in Greater Paris, the figure was almost 40% of all deaths from early March to late May. The weekly peak mortality due to Covid-19 is comparable to the record hot summer of 2003 (see graph below).
Didier Raoult, a well-known professor of medicine and HCQ pioneer from Marseille, criticized the lack of early treatment and the ban on HCQ at a parliamentary hearing at the end of June. Until 2019, HCQ was available in France without prescription. At the beginning of the pandemic, however, its use was restricted to clinics and eventually banned altogether. The reason for the ban was the falsified Lancet study from the end of May (which was later retracted).
In his clinic, Prof. Raoult had been able to reduce the case fatality rate to a very low 0.9% by early treatment with HCQ, according to a published retrospective analysis.




Charts and report: Santé Public France
Germany
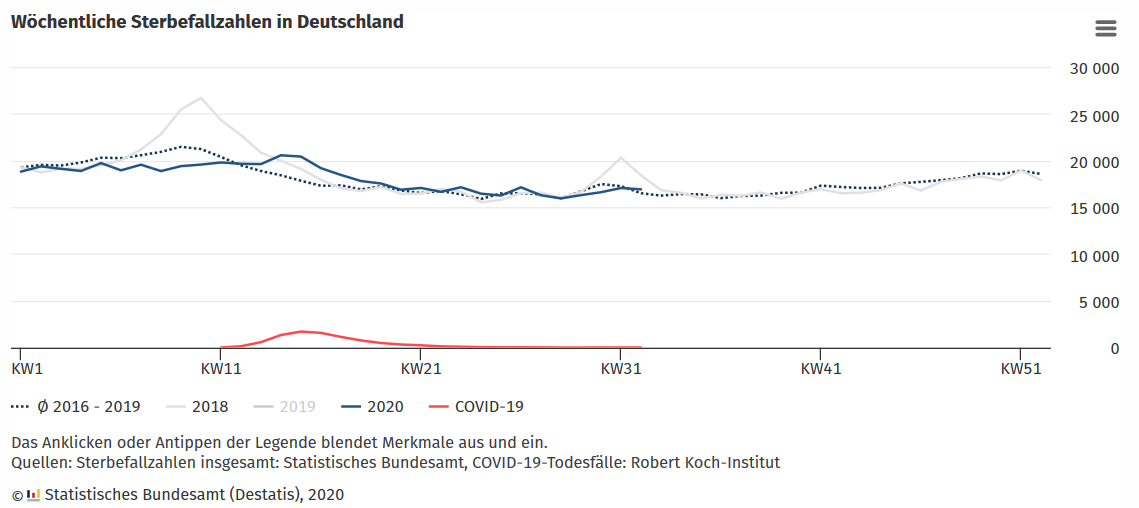
Germany counts only about 9000 corona deaths and has not experienced any significant excess mortality (in population-adjusted terms there was even a slight undermortality).
At the end of June, however, only 1.3% of blood donors had IgG antibodies against the new coronavirus. This value is very low. Even if non-blood donors (including children and sick persons), T-cells and mucosal (IgA) immunity are taken into account, exposure of the population to the virus is hardly more than 10% to 15%.
This means that the new coronavirus has not yet spread widely in Germany. The measures or – more likely – the anticipation of the measures by the population therefore seem to have been “successful” in this sense (see graph below).
On the other hand, this means that epidemiologically, Germany is essentially still where it was in April and that the risk of a new and stronger increase in infections and disease is indeed real. The comparison with France shows what this can entail.
The German government currently seems to be following a suppression and vaccination strategy. This strategy is socially and economically costly and its success remains uncertain. As an alternative or addition, an early treatment concept should be examined.
The political corona situation in Germany remains tense. Repeatedly, sanctions have been imposed on doctors, professors, lawyers and civil servants who are critical of corona, and in some cases serious attacks occurred against skeptical journalists and activists.
Since June, an extra-parliamentary committee of inquiry consisting of lawyers and medical experts has been dealing with the German Corona government policy. It should not be forgotten, however, that the corona pandemic in Germany is probably not yet over, given that by the end of June, only 1.3% of blood donors had IgG antibodies against the virus.
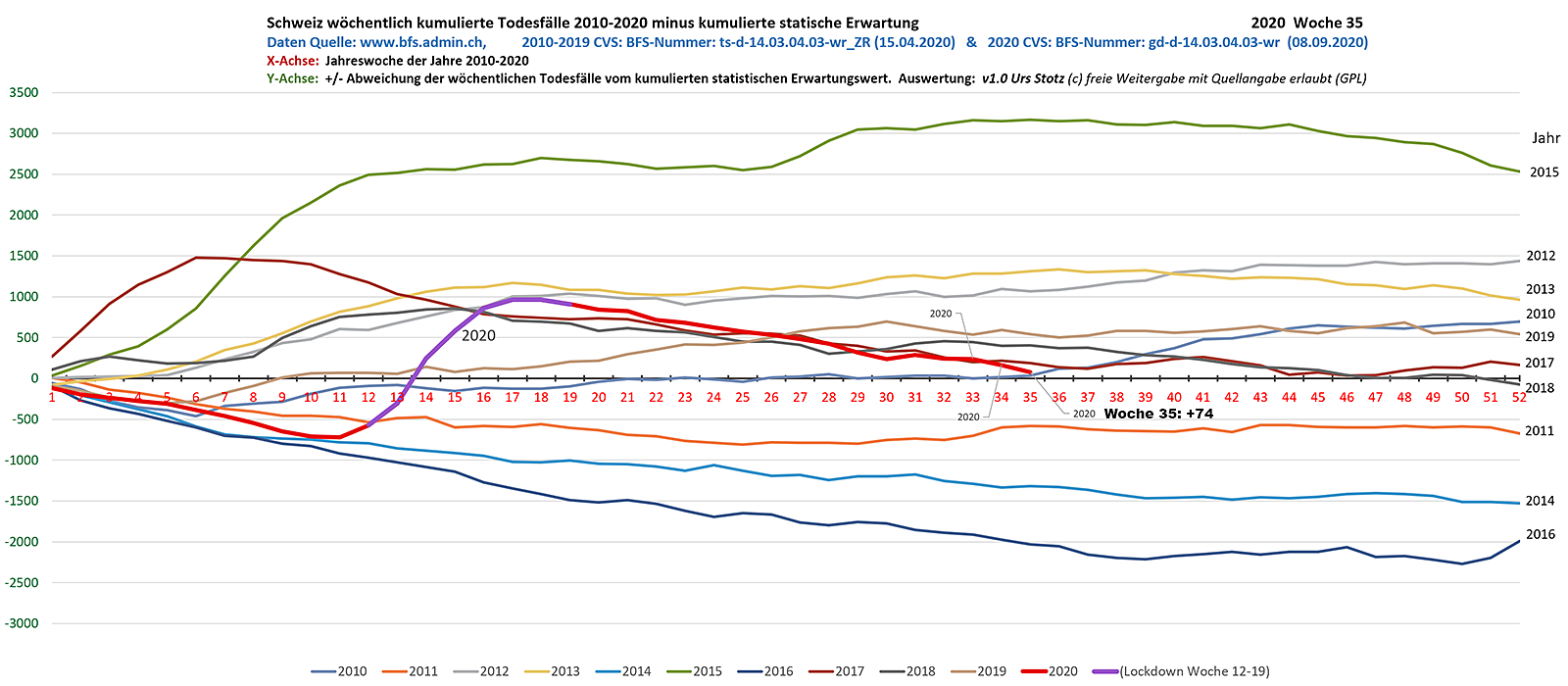
Switzerland
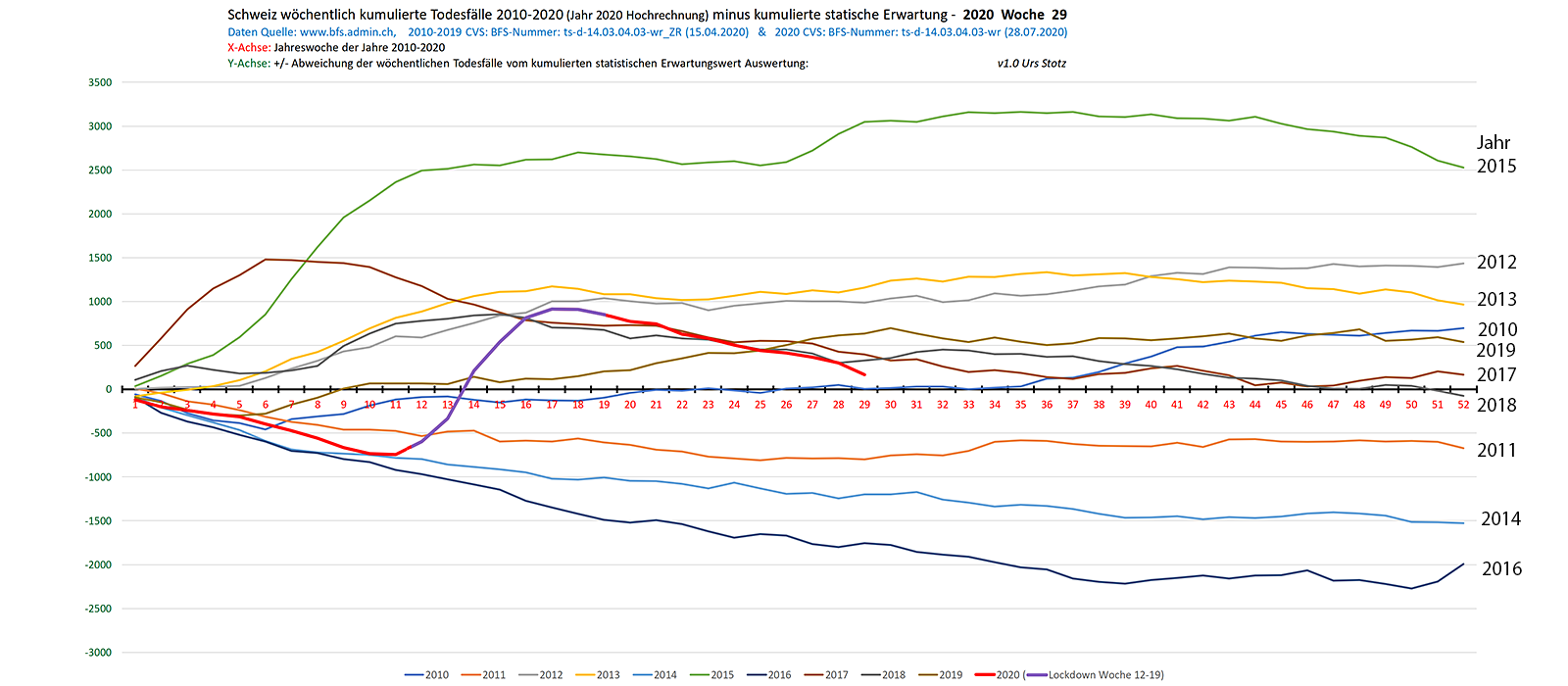
- The Swiss annual excess mortality is currently close to zero (see graph), which is below most flu waves of the last ten years. This is due to the mild winter and the very high median age of the approximately 1700 corona deaths (84 years). About 50% of the deaths occurred in nursing homes. The effect of the lockdown remains questionable.
- In the former hotspots Ticino and Geneva, IgG antibody levels in May were about 10%, about ten times higher than found by daily PCR tests. Taking mucosal and cellular immunity into account, exposure in southern and western Switzerland could already be around 50%. In German-speaking Switzerland, however, exposure is likely to be lower. The risk of a “second wave” is therefore real.
- In principle, the Swiss government is pursuing a suppression and vaccination strategy, which it is supplementing with mass testing, contact tracing and compulsory masking. As an alternative, infectiologist Dr. Pietro Vernazza brought up the idea of controlled exposure with protection of risk groups based on the Swedish model.
- Switzerland still has no early treatment strategy and thus risks an unnecessarily high hospitalisation and death rate.
- Sweden and Belarus, both of which managed the corona pandemic without a lockdown and without compulsory masks, have been removed from the Swiss list of “high-risk countries” in mid-July. Sweden had previously put Switzerland on its own high-risk list. In fact, the increase in Swedish “cases” was solely due to an increase in tests.
- A referendum was launched against the corona tracing app “SwissCovid”. The initiators are raising data protection and security concerns. Previously, Swiss Professor Serge Vaudenay published a critical analysis of the app, which isn’t as transparent as claimed, leaving Google and Apple in control, Vaudenay said.
- A referendum is also being prepared against the Swiss “Covid-19 Law”, which extends the Corona emergency law until the end of 2022. In addition, a petition has been launched calling for an extra-parliamentary commission of inquiry into the corona measures.
- A flyer campaign against the compulsory use of masks in public transport also caused a stir. The director of the BAG hastily called the arguments of the critics “fake news”.
- Infosperber: The Covid-19 task force massively exaggerated the benefits of masks
- For more current and critical corona analyses see corona-transition.org
Sweden
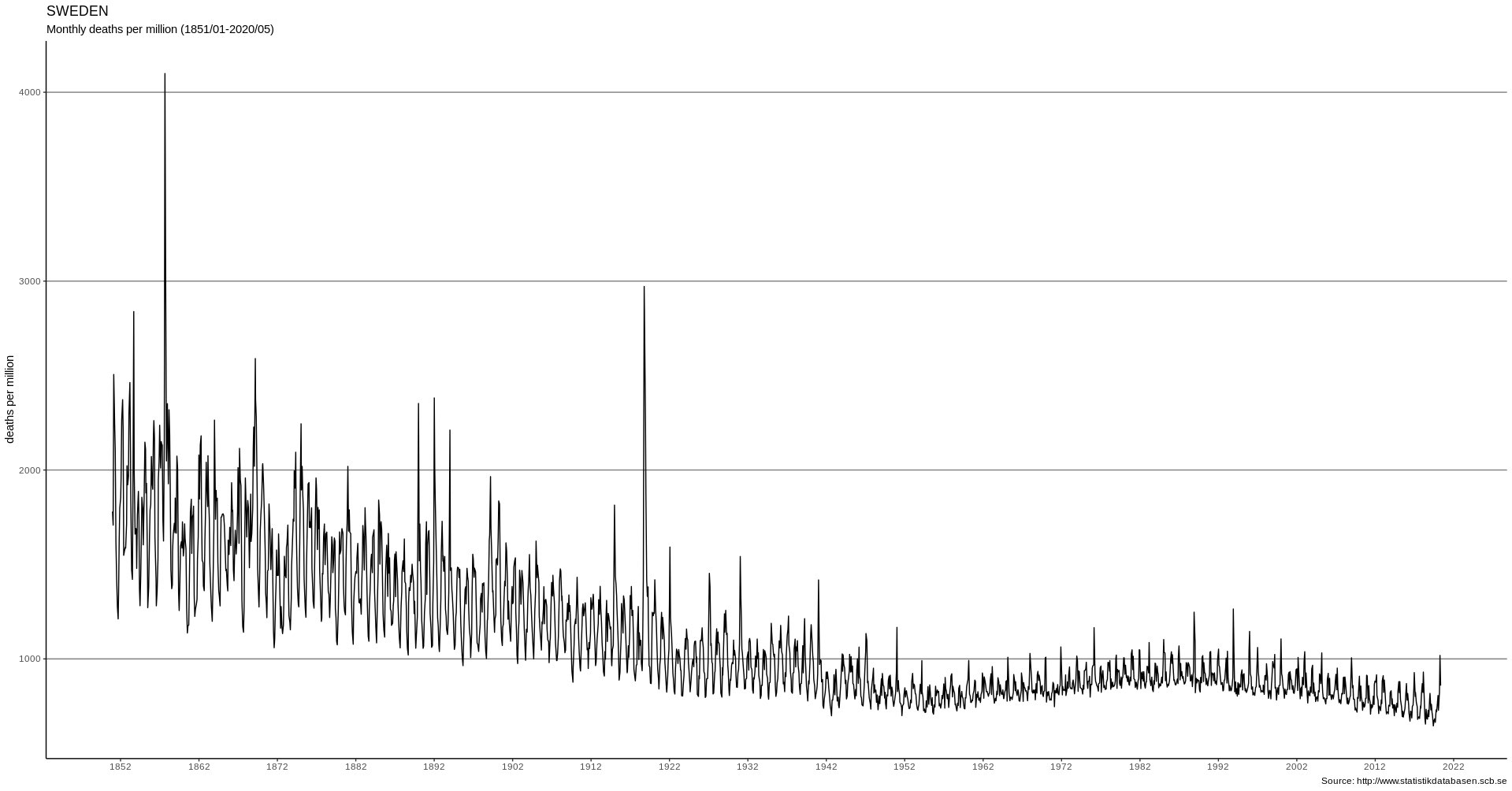
- In Sweden, daily corona deaths are now close to zero. The overall mortality rate is in the range of earlier strong flu waves. Even the monthly peak mortality (in April 2020) remained below the strong flu waves of the 1990s.
- The example of Sweden (and Belarus) shows that a lockdown was not necessary if the population and institutions were well prepared. However, from the perspective of many lockdown advocates – governments and the media – this is very difficult to admit.
- Sweden is one of the few Western countries that – on the basis of the medical evidence – has not closed its primary schools. This decision was correct, too.
- Sweden made two real mistakes, which ironically are not covered by most of the media: 1) The nursing homes in the Stockholm area were protected too late and caused over 50% of Swedish deaths. 2) Sweden had no early treatment strategy that could have reduced the hospitalisation and death rates.
- Swedish cities showed an IgG antibody prevalence between 10% and 20% in July, which, together with mucosal and cellular immunity, indicates that the population was exposed between 50% and 100%. Sweden is therefore probably the best placed of all western countries to start the coming winter.
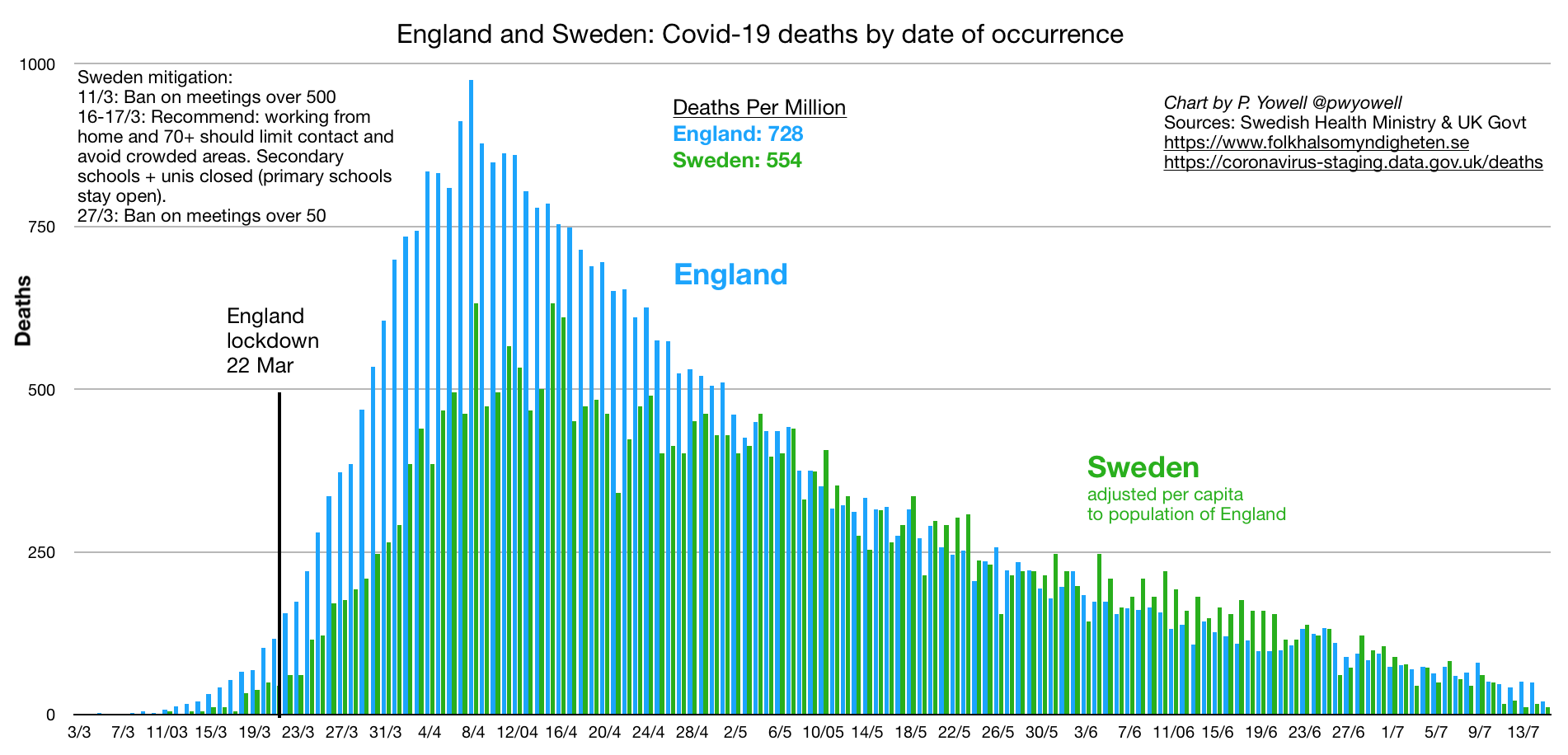
The following graphs compare the deaths in Sweden with those in England and New York.

Charts: Paul Yowell
India
India, which relies on early treatment and even prophylaxis with the antimalarial drug HCQ, officially counts only about 35,000 corona deaths among its 1.3 billion people.
An Indian antibody study came to the conclusion that around 23% of the 20 million inhabitants of the Indian capital Delhi already have antibodies against the new corona virus. This is about 35 times more people than confirmed by PCR tests.
This means that Delhi (and some other major cities) could already be beyond or near the herd immunity threshold, taking into account mucosal and cellular immunity.
Latin America
Brazil has by now suffered 90,000 Covid deaths and thus ranges between the Netherlands and France in terms of deaths per population. In the meantime, Brazil has introduced an early treatment concept based on zinc and HCQ.
Chile and Peru currently have an even higher death rate than Brazil (based on population). With close to 20,000 deaths, Peru is in the range of Italy and Spain.
C. Political notes
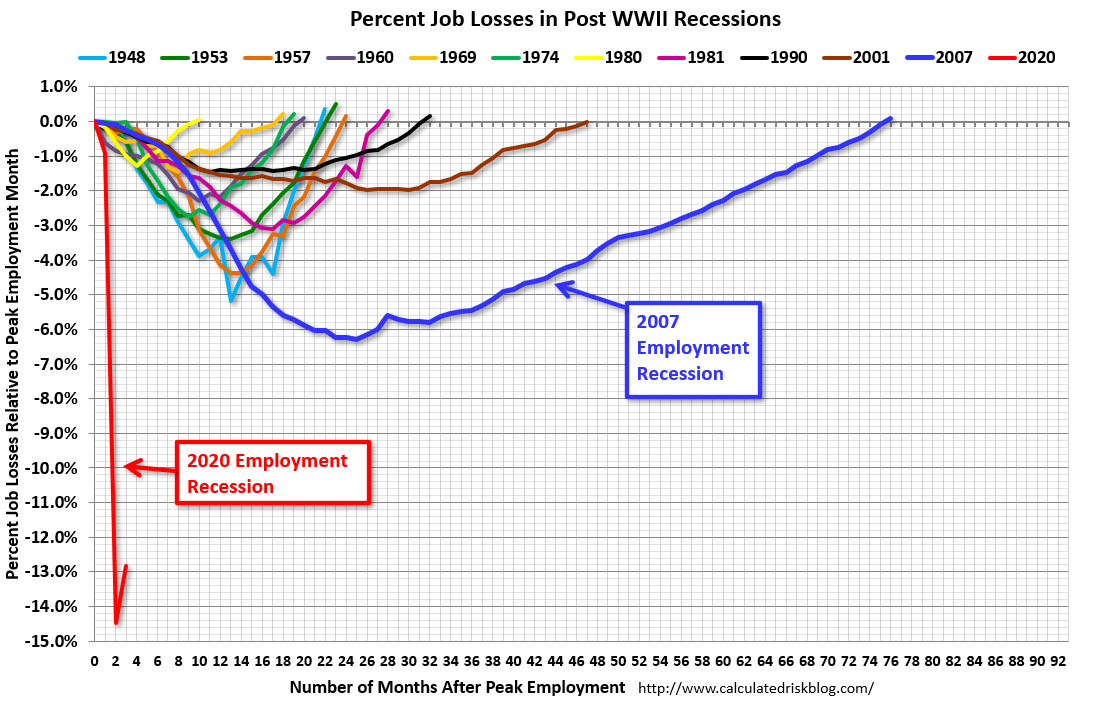
- The US economy contracted by an annualized 32.9% in the second quarter, the highest rate since 1947. The second highest decline was in 1958 (10%) – in the wake of the Asian flu pandemic.
- In the US, up to 28 million people might lose their homes due to corona lockdowns and the economic downturn, which could trigger a new mortgage crisis.
- The German economy contracted by 10.1% in the second quarter compared with the same quarter of the previous year – the biggest decline since 1970.
- According to the UN, the corona lockdowns and the global economic depression could plunge up to 225 million people worldwide into a famine by the end of the year.
- The EU Commission demands or plans the “networking” of national corona tracing apps.
- The NGO Privacy International warns of a “looming disaster” with immunity passports and digital identity cards.
- The authoritarian government of Turkmenistan apparently banned the use of the word “coronavirus”. Consequently, there are no coronavirus deaths in the country, at least officially. Those who wear a mask are arrested by police, Reporters without Borders said.
July 2020
On the development of the pandemic
In most Western countries, the peak of coronavirus infections was already reached in March or April and often before the lockdown. The peak of deaths in most Western countries was in April. Since then, hospitalizations and deaths have been declining in most Western countries (see graphs below).
This development also applies to countries without a lockdown, such as Sweden, Belarus and Japan. Cumulative annual mortality in most western countries continues to be in the range of a mild (e.g. CH, AT, DE) to strong (e.g. USA, UK) influenza season.
After the end of the lockdowns, the number of corona tests in the low-risk general population has increased strongly in many countries, for example in connection with people returning to work and school.
This led to a certain increase in positive test results in some countries or regions, which was portrayed by many media and authorities as an allegedly dangerous increase in “case numbers” and sometimes led to new restrictions, even if the rate of positive tests remained very low.
“Case numbers” are, however, a misleading figure that cannot be equated with sick or infected people. A positive test can, for example, be due to non-infectious virus fragments, an asymptomatic infection, a repeated test, or a false-positive result.
Moreover, counting alleged “case numbers” is not meaningful simply because antibody tests and immunological tests have long shown that the new coronavirus is up to fifty times more widespread than assumed on the basis of daily PCR tests.
Rather, the decisive figures are the number of sick people, hospitalisations and deaths. It should be noted, however, that many hospitals are now back to normal operation and all patients, including asymptomatic patients, are additionally tested for the coronavirus. Therefore, what matters is the number of actual Covid patients in hospitals and ICUs.
In the case of Sweden, for example, the WHO had to withdraw the classification as a “risk country” after it became clear that the apparent increase in “cases” was due to an increase in testing. In fact, hospitalisations and deaths in Sweden have been declining since April.
Some countries have already been in a state of below-average mortality since May. The reason for this is that the median age of corona deaths was often higher than the average life expectancy, as up to 80% of deaths occurred in nursing homes.
In countries and regions where the spread of the coronavirus has so far been greatly reduced, it is nevertheless entirely possible that there will be a renewed increase in Covid patients. In these cases, early and effective treatment is important (see below).
Global Covid-19 mortality is currently – despite the significantly older population nowadays – a whole order of magnitude below the flu pandemics of 1957 (Asian flu) and 1968 (Hong Kong flu) and in the range of the rather mild “swine flu pandemic” of 2009.
The following charts illustrate the discrepancy between “cases” and deaths:



The following charts compare Covid mortalities to earlier flu seasons (more):


The following chart compares deaths in Sweden (no lockdown) New York State:
The following chart compares the Covid-19 pandemic to earlier pandemics:
On the lethality of Covid-19
Most antibody studies have shown a population-based Infection Fatality Rate (IFR) of 0.1% to 0.3%. The US health authority CDC published in May a still cautious “best estimate” of 0.26% (based on 35% asymptomatic cases).
At the end of May, however, an immunological study by the University of Zurich was published, which for the first time showed that the usual antibody tests that measure antibodies in the blood (IgG and IgM) can detect at most about one fifth of all coronavirus infections.
The reason for this is that in most people the new coronavirus is already neutralised by antibodies on the mucous membrane (IgA) or by cellular immunity (T cells) and no symptoms or only mild symptoms develop.
This means that the new coronavirus is probably much more widespread than previously assumed and the lethality per infection is around five times lower than previously estimated. The real lethality could therefore be significantly below 0.1% and thus in the range of influenza.
At the same time, the Swiss study may explain why children usually develop no symptoms (due to frequent contact with previous corona cold viruses), and why even hotspots such as New York City found an antibody prevalence (IgG/IgM) of at most 20% – as this already corresponds to herd immunity.
The Swiss study has in the meantime been confirmed by several more studies:
- A Swedish study showed that people with mild or asymptomatic disease often neutralized the virus with T-cells without the need to produce antibodies. Overall, T-cell immunity was about twice as common as antibody immunity.
- A large Spanish antibody study published in Lancet showed that less than 20% of symptomatic people and about 2% of asymptomatic people had IgG antibodies.
- A German study (preprint) showed that 81% of the people who had not yet had contact with the new corona virus already had cross-reactive T-cells and thus a certain background immunity (due to contact with previous corona cold viruses).
- A Chinese study in the journal Nature showed that in 40% of asymptomatic persons and in 12.9% of symptomatic persons no IgG antibodies are detectable after the recovery phase.
- Another Chinese study with almost 25,000 clinic employees in Wuhan showed that at most one fifth of the presumably infected employees had IgG antibodies (press article).
- A small French study (preprint) showed that six of eight infected family members of Covid patients developed a temporary T-cell immunity without antibodies.
Video interview: Swedish Doctor: T-cell immunity and the truth about Covid-19 in Sweden
In this context, a US study in the journal Science Translational Medicine, using various indicators, concluded that the lethality of Covid-19 was much lower than originally assumed, but that its spread in some hotspots was up to 80 times faster than suspected, which would explain the rapid but short-duration increase in patients.
A study in the Austrian ski resort of Ischgl, one of the first European “corona hotspots”, found antibodies in 42% of the population. 85% of the infections went “unnoticed” (i.e. very mild), about 50% of the infections went completely without (noticeable) symptoms.
The high antibody value of 42% in Ischgl was due to the fact that Ischgl also tested for IgA antibodies in the blood (instead of only IgM/IgG). Additional tests for mucosal IgA and for T-cells would undoubtedly have shown even higher immunity levels close to herd immunity.
Ischgl saw two Covid-related deaths (both of them men over 80 with preconditions), resulting in a ‘crude IFR’ of 0.26%. Considering the population structure and the actual extent of immunity, the population-based Covid lethality is likely to be below 0.1%
Due to its rather low lethality, Covid-19 falls at most into level 2 of the five-level pandemic plan developed by US health authorities. For this level, only the “voluntary isolation of sick people” is to be applied, while further measures such as face masks, school closings, distance rules, contact tracing, vaccinations and lockdowns of entire societies are not recommended.
The new immunological results also mean that “immunity passports” and mass vaccinations are unlikely to work and are therefore not a useful strategy.
Some media continue to speak of allegedly much higher Covid lethality levels. However, these media refer to outdated simulation models, confuse mortality and lethality, or CFR and IFR, or “raw IFR” and population-based IFR. More about these errors here.
In July, an antibody prevalence of allegedly up to 70% was reported in some New York City districts. However, this is not a population-based figure, but rather antibodies in people who had visited an urgent care center.
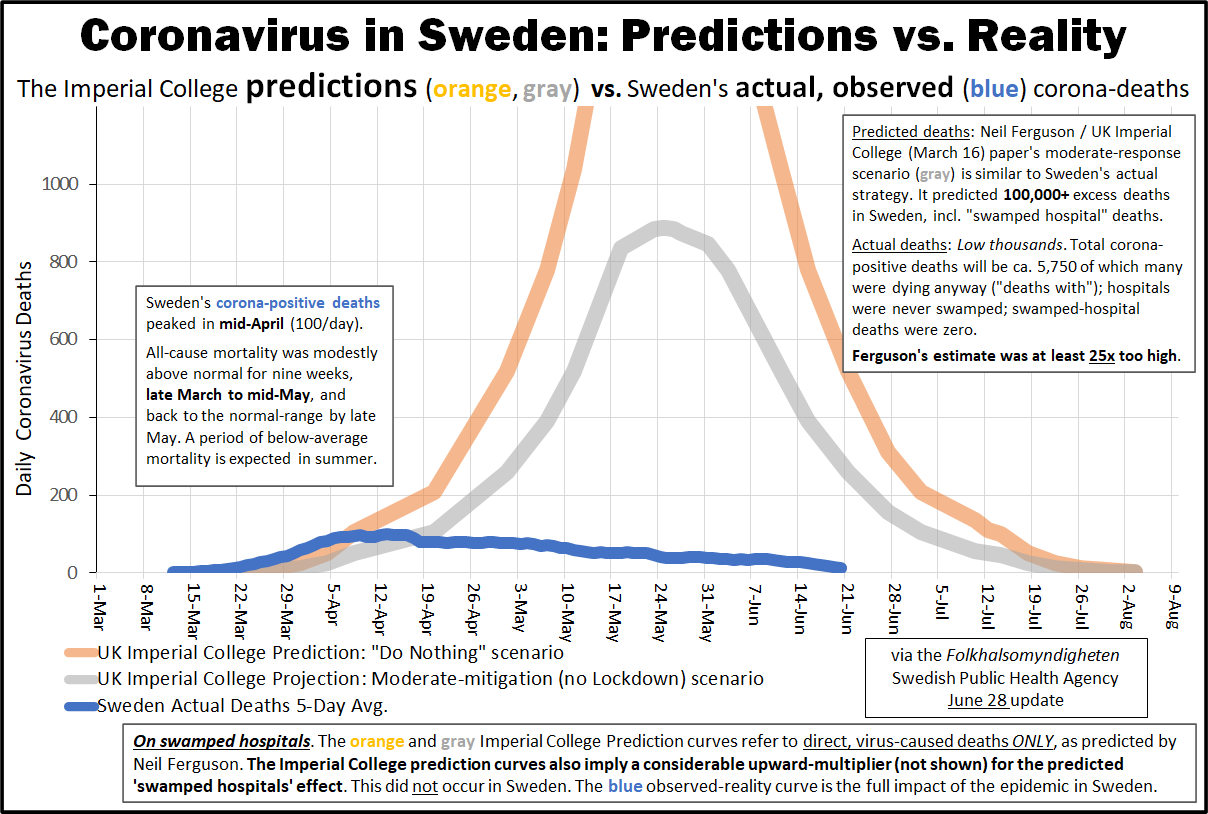
The following graph shows the actual development of corona deaths in Sweden (no lockdown, no face mask obligation) compared to the forecasts of Imperial College London (orange: no measures; grey: moderate measures). Swedish annual all-cause mortality actually is in the range of a medium flu wave and 3.6% lower than in previous years.
On the health risks of Covid-19
Why is the new coronavirus harmless for many people, but very dangerous for some people? The reason has to to with special features of the virus and the human immune system.
Many people, including almost all children, can neutralise the new corona virus with an existing immunity (due to contact with previous corona cold viruses) or through antibodies on the mucous membranes (IgA), without it causing much damage.
However, if this does not succeed, the virus can penetrate the organism. There the virus can cause complications in the lung (pneumonia), the blood vessels (thromboses, embolisms), and other organs due to its efficient use of the human ACE2 cell receptor.
If in this case the immune system reacts too weakly (in older people) or too strongly (in some younger people), the course of the disease can become critical.
It has also been confirmed that the symptoms or complications of serious Covid-19 disease can last for weeks or even months in some cases.
Therefore, the new coronavirus should not be underestimated and early and effective treatment is absolutely crucial for patients at risk.
In the longer term, the new coronavirus could develop into a typical cold virus, similar to the coronavirus NL63, which also uses the ACE2 cell receptor and nowadays affects primarily young children and nursing patients, causing upper and lower respiratory tract infections.
On the treatment of Covid-19
Note: Patients are asked to consult a doctor.
Several studies have now confirmed what some front-line physicians have been saying since March: Early treatment of Covid patients with zinc and the malaria drug hydroxychloroquine (HCQ) is indeed effective. US doctors have reported a reduction in hospitalisation rates of up to 84% and a stabilisation of the health condition often within a few hours.
Zinc has antiviral properties, HCQ supports zinc absorption and has additional antiviral properties. These drugs are supplemented by doctors if necessary with an antibiotic (to prevent a bacterial superinfection) and a blood thinner (to prevent infection-related thromboses and embolisms).
The alleged or actual negative results with HCQ in some studies were based, according to the current state of knowledge, on delayed use (intensive care patients), excessive doses (up to 2400mg per day), manipulated data sets, or ignored contraindications (e.g., favism or heart problems).
Sadly, the WHO, many media and some authorities may have caused considerable and unnecessary damage to public health in recent months through their negative stance, which may have been politically motivated or influenced by pharmaceutical interests.
French professor of medicine Jaouad Zemmouri, for example, estimates that Europe could have avoided up to 78% of Covid deaths by adopting a consistent HCQ treatment strategy.
HCQ contraindications such as favism or heart problems need to be considered, but the recent Ford Medical Center study achieved a reduction in hospital deaths of around 50% even with 56% African-American patients (who more often have favism).
However, the crucial point in the treatment of high-risk patients is early intervention as soon as the first typical symptoms develop and even without a PCR test in order to prevent progression of the disease and avoid intensive care hospitalization.
Most countries did the exact opposite: after the infection wave in March, they imposed a lockdown, so that infected and frightened people were locked up in their homes without treatment and often waited until they developed severe respiratory distress and had to be taken directly to the intensive care unit, where they were often sedated and intubated and were likely to die.
It is conceivable that a zinc HCQ combination protocol, which is simple, safe and inexpensive, could make more complex drugs, vaccinations and measures largely obsolete.
More recently, a case study from France showed that in four of the first five patients treated with the much more expensive drug Remdesivir from the pharmaceutical company Gilead, treatment had to be discontinued due to liver issues and kidney failure.
Read more: On the treatment of Covid-19
On the effectiveness of masks
Various countries have introduced or are currently discussing the introduction of mandatory masks in public transport, in shopping malls, or generally in public.
Some may argue that the discussion has become largely obsolete because of the lower-than-expected lethality and hospitalization rate of Covid-19 and the available treatment options, which have mostly eased the initial concern of “flattening the curve”.
Nevertheless, the question of the effectiveness of masks can be asked. In the case of influenza epidemics, the answer is already clear from a scientific point of view: masks in everyday life have no or very little effect. If used improperly, they can even increase the risk of infection.
Ironically, the best and most recent example of this is the often-mentioned Japan: Despite its ubiquitous masks, Japan experienced its most recent strong flu wave – with around five million people falling ill – just one year ago, in January and February 2019.
However, unlike SARS corona viruses, influenza viruses are transmitted also by children. Indeed, Japan had to close around ten thousand schools in 2019 due to acute outbreaks of the flu.
With the SARS 1 virus of 2002 and 2003, there is some evidence that medical masks can provide partial protection against infection. But SARS-1 spread almost exclusively in hospitals, i.e. in a professional environment, and hardly to the general public at large.
In contrast, a study from 2015 showed that the cloth masks in use today are permeable to 97% of viral particles due to their pore size and can further increase the risk of infection by storing moisture.
Some studies recently argued that everyday masks are nevertheless effective in the case of the new coronavirus and could at least prevent the infection of other people. However, these studies suffer from poor methodology and sometimes show the opposite of what they claim.
Typically, these studies ignore the effect of other simultaneous measures, the natural development of infection numbers, changes in test activity, or they compare countries with very different conditions.
An overview:
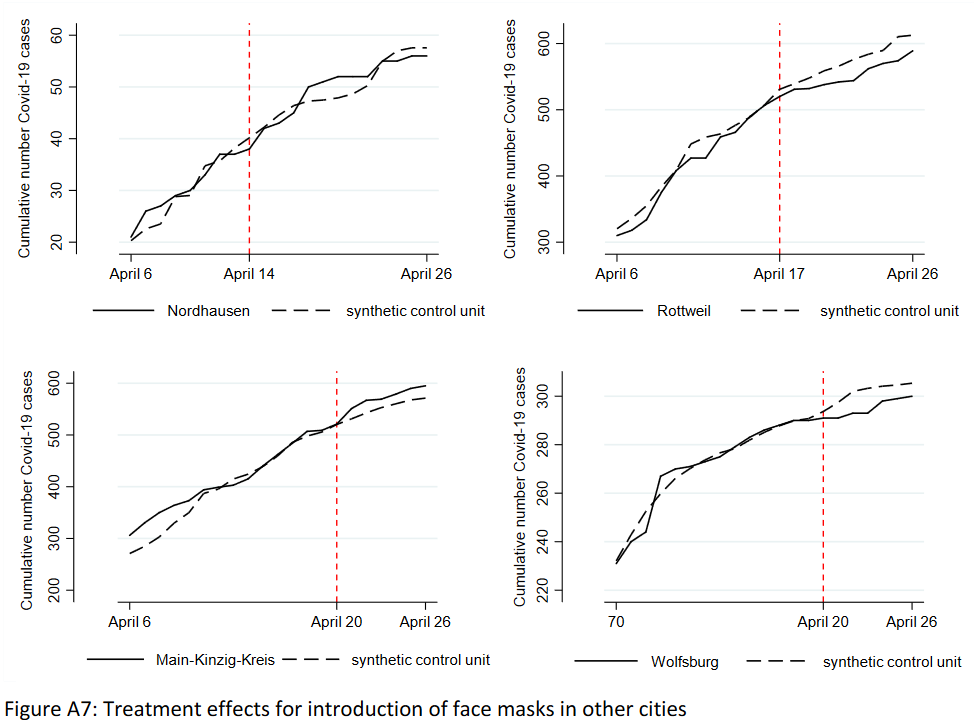
- A German study claimed that the introduction of compulsory masks in German cities had led to a decrease in infections. But the data does not support this: in some cities there was no change, in others a decrease, in others an increase in infections (see graph below). The city of Jena, presented as a model, simultaneously introduced the strictest quarantine rules in Germany, but the study did not mention this.
- A study in the journal PNAS claimed that masks had led to a decrease in infections in three hotspots (including New York City). This did not take into account the natural decrease in infections and other measures. The study was so flawed that over 40 scientists recommended that the study be withdrawn.
- A US study claimed that compulsory masks had led to a decrease in infections in 15 states. The study did not take into account that the incidence of infection was already declining in most states at that time. A comparison with other states was not made.
- A Canadian study claimed that countries with compulsory masks had fewer deaths than countries without compulsory masks. But the study compared African, Latin American, Asian and Eastern European countries with very different infection rates and population structures.
- A meta-study in the journal Lancet claimed that masks “could” lead to a reduction in the risk of infection, but the studies considered mainly hospitals (Sars-1) and the strength of the evidence was reported as “low”.
The medical benefit of compulsory masks therefore continues to remain questionable. A comparative study by the University of East Anglia, for instance, came to the conclusion that compulsory masks had no measurable effect on the incidence of Covid infections or deaths.
It is also clear that widespread use of face masks couldn’t stop the initial outbreak in Wuhan.
Sweden showed that even without a lockdown, without mandatory masks and with one of the lowest intensive care bed capacities in Europe, hospitals need not be overburdened. In fact, Sweden’s annual all-cause mortality has remained in the range of previous flu seasons.
At any rate, authorities shouldn’t suggest to the population that mandatory masks reduce the risk of infection, for example in public transport, as there is no evidence of this. Whether with or without masks, there is an increased risk of infection in densely packed indoor areas.
Interestingly, the demand for a worldwide obligation to wear masks is led by a lobby group called “masks4all” (masks for all), which was founded by a “young leader” of the Davos forum.
The role of contact tracing
Numerous countries have introduced smartphone apps and special units for “contact tracing”. However, there is no evidence that these can make an epidemiologically relevant contribution.
In the case of tracing pioneer Iceland, the app has largely failed, in Norway it was stopped for data protection reasons, in India, Argentina, Singapore and other countries it became mandatory after all, in Israel contact tracing is operated directly by the secret service.
A WHO study on influenza pandemics in 2019 came to the conclusion that contact tracing is not useful from an epidemiological point of view and “is not recommended in any circumstances”. The typical area of application is rather sexually transmitted diseases or food poisoning.
Moreover, serious concerns about data protection and civil rights remain.
NSA whistleblower Edward Snowden warned as early as March that governments could use the corona crisis as an occasion or pretext for expanding global surveillance and control, thus creating an “architecture of oppression”.
A whistleblower who had taken part in a training program for contact tracers in the US described it as “totalitarian” and a “danger to society”.
Swiss computer science professor Serge Vaudenay showed that the contact tracing protocols are by no means “decentralized” and “transparent”, because the actual functionality is implemented through a Google and Apple interface (GAEN) that is not “open source”.
This interface has now been integrated by Google and Apple into three billion mobile phones. According to Prof. Vaudenay, the interface may record and store all contacts, not just those that are medically “relevant”. A German IT expert, for his part, described tracing apps as a “Trojan horse”.
For more information on “contact tracing”, see the June update.
See also: Inside the NSA’s Secret Tool for Mapping Your Social Network (Wired)

On the origin of the new coronavirus
In the June update it was shown that renowned virologists consider a laboratory origin of the new coronavirus to be “at least as plausible” as a natural origin. This is due to some genetic peculiarities of the virus in the receptor binding domain, which lead to high infectivity in humans.
In the meantime, further evidence for this hypothesis has emerged. More in these articles:
- Covid-19 Virus Origin: The Mojiang Miners Passage Hypothesis (SPR)
- Seven year coronavirus trail from bat cave via Wuhan lab (London Times)
- Pentagon biolab discovered MERS and SARS-like coronaviruses in bats (DG)
Developments since the beginning of 2020 show that the new coronavirus cannot be seen as a “bioweapon” in the strict sense of the term, as it is not deadly enough and not targeted enough. However, it may well cause fear among the population and be exploited politically.
Nevertheless, besides a potential lab origin, a natural origin continues to be a realistic possibility, even though the “Wuhan wet market” hypothesis and more recently the pangolin hypothesis have in the meantime been ruled out by experts.
Continue to previous updates →
__________________________________________
![]() Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Languages: AR, CN, CZ, DE, EN, EO, ES, FR, GR, HE, HU, IT, JP, KO, MS, NL, NO, PL, PT, RO, RU, SE, TR
Tags: Airborne contagion, COVID-19, China, Community, Compassion, Coronavirus, Cuba, Economy, Empathy, Environment, Health, Lockdown, Orthomolecular Medicine, Pandemic, Public Health, Research, Science, Science and Medicine, Swiss Policy Research, United Nations, WHO
DISCLAIMER: The statements, views and opinions expressed in pieces republished here are solely those of the authors and do not necessarily represent those of TMS. In accordance with title 17 U.S.C. section 107, this material is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. TMS has no affiliation whatsoever with the originator of this article nor is TMS endorsed or sponsored by the originator. “GO TO ORIGINAL” links are provided as a convenience to our readers and allow for verification of authenticity. However, as originating pages are often updated by their originating host sites, the versions posted may not match the versions our readers view when clicking the “GO TO ORIGINAL” links. This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more information go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
One Response to “Facts about Covid-19”
Read more
Click here to go to the current weekly digest or pick another article:
COVID19 - CORONAVIRUS:
[…] latest immunological studies show Covid lethality at 0.1% to 0.5% in most countries. From a historical perspective, Covid is far […]