
Homogenization of Psychotherapy and Counseling: Scientific, Professional, Ethical/Moral Issues, Risks, and Directions
TRANSCEND MEMBERS, 30 Apr 2018
Anthony J. Marsella, Ph.D. – TRANSCEND Media Service
Homogenization: Efforts Pursuing Standardization, Control, Domination, Oppression!
28 Apr 2018 – I am gravely concerned and fearful by the widespread pursuit and endorsement of homogenization in many sectors of our life. I am particularly concerned about the consequences homogenization may have for “robotic-like” existence for human beings, limiting opportunity, and diversity.
Trade-Offs
Homogenization is rooted in “standardization!” “Standardization” offers certain protections against extremes in variation capable of harming individuals and groups. At the same time, “standardization” results in dominance, control, and oppression. “Standardization” resists variations associated with growth, change, diversity. Some say, standardization is a “trade-off;” and this is difficult to deny. But, there are risks. The caveat may reside in recognizing the “trade-offs,” and identifying the risk-benefit tradeoff.
For example, homogenization in education often fails to acknowledge individual or group variations, not only in abilities and talents, but also the contributions of gender, ethnocultural, and racial differences. At this point it is a win-lose situation. “Standardization,” with pressures for uniformity in education goals, methods, and outcomes, risks losing lives by the very institution designed to develop and nurture individual and group potential.
Clearly, there are areas in which standardization has utility and value, including certain medical surgical procedures, airline pilot training, equipment, training, and related performance-based technologies. Even in these examples, however, we must question the tendency for contentment with specified goals and procedures, and while resisting other options. There must be, in my opinion, a tolerance for change, rooted in a constant evaluation of consequences.
Acculturation is Omnipresent
I believe we must maintain a commitment to diversity, (i.e., “Life is Diversity”), and recognize homogenization presents problems stifling creativity and innovation in favor of accepted standards. Too often, an existing power structure (group, cabal, cartel) retains control by reducing or eliminating contrary view or positions.
I grew up and was socialized in a traditional Sicilian immigrant household; I as I went to school, I was caught between two worlds. Some resolution occurred as I discovered: selective detachment! I did not have to buy into the entire ways-of-life. I could choose based on situations and perceived consequences. Freedom! I must add however, resolution requires compromise, and compromise can be traced to existing power distribution. Should Amazon tribes acculturate? Should spouses acculturate?
Evidence-Based Homogenization of Therapies and Counseling
Energetic efforts are in progress to develop and canonize a recommended “menu” of evidence–based therapies acceptable for application and implementation.
A major issue is: acceptable and implementation for who? Under the guise of “scientific” evaluation standards, the recommended “menu” poses serious risks and problems for both patient and therapist.
- Legal Issues:
Both insurance systems and conventional professional organizations support these efforts. Insurance systems are seeking a “legal” basis for reimbursement of psychotherapy and counseling services which would help them approve and disapprove petitions for reimbursement.
- Financial Issues:
Clearly, as cries for mental health services increase in the wake of mass violence and deaths related to societal and cultural collapse, innocent victims are increasing. In addition, financial costs for mental health interventions therapy are experiencing an alarming rise, and serious limitations in quality of care. For insurance systems, private and public, the costs pose a challenge for profits.
- Professional-Cabal Interests
In addition to insurance systems, conventional professional mental health-related organizations and providers are seeking to legitimize practices under the rubric of “evidence-based” standards. Existing professional groups favoriting certain procedures, and codifying them in journals, programs, funding sources also represent a source of problems.
Some groups currently dominating “acceptable” conventional views favor specific histories, assumptions, methods, procedures, and outcome data. These groups may control journal research methods, and book publications, often times based on an “empirical” foundation for preferred teaching, research, and applications.
“Science” as Arbiter
Here we must also remember “empiricism” does not mean “scientific,” and “scientific” does not mean bias-free. Most professionals are aware “power, position, and person often determine canon. This is true in medicine, physics, economics, and education; it is also true in mental health. I shudder as I hear politicians seeking approval call for increases in mental health services without recognizing the numerous limitations and issues in mental health care.
Let me be clear in my purposes: I am not speaking against inquiry, nor research of any ilk, for exploring the “successes” or “cures” in psychotherapy and counseling. I am, however, critical of efforts after homogenization and uniformity in an area begging for recognition of variability and resisting imposition of set standards under the risk of financial and ethical violations for non-compliance.
The fact of the matter is conventional mental health institutions and practices have strong ideological attachment supported by uniformity, conformity, and compliance with certain assumption and procedures. In a world now dominated by surveillance, monitoring, and archiving of virtually every aspect of our lives for purposes of “commercial” and “national” security, efforts after yet more “standardization” related to cures and healing assume our knowledge is accurate.
Homogenization brings uniformity, and uniformity brings compliance, and compliance brings control. It is an issue of “En Loco Parentis.” Further, a have come to believe one task of psychotherapy and counseling may be to introduce an understanding of how power and authority in lives are problems sources! Liberation therapy?
To all of these ends, I wish to discuss critiques and knowledge-information material for consideration: (1) Mental Health; (2) Mental Health Industry; (3) Outcome Uniformity Equation; (4) Non-Western Therapies; (5) Healing Principles; (6) Quo Vadis?
Mental Health: Issues
- Mental Health Industry
There is a vast mental health industrial complex exacting control over definitions of mental health and the legitimacy of practices ranging from diagnosis/classification to therapies and prevention.
I wonder if most are aware of the industry nature of the field. Table 1 lists members of the mental health industry complex:
Table 1: Mental Health Professions, Professionals and Technical-Support Services (Marsella, 2016)
- Clinical Nurse Specialist (MSN)
- Clinical Psychologist (Ph.D. or D.Psy.)
- Counseling Psychologist (D.Ed., Ph.D., D.Psy.)
- Drug Counselor (Varies)
- Family Advocacy Groups
- Licensed Psychologist (Ph.D. Non-clinical)
- Licensed Practical Nurse (LPN)
- Marriage and Family Therapists (MFT)
- Medical Intern (M.D.)
- Mental Health Aide (Certificate or Diploma)
- Occupational Therapist (O.T. Degree, License, Certificate)
- Pastoral Counselor (Varies)
- Physician (M.D. or O.D. + Internship and Medical Residency)
- Psychiatrist (M.D. or O.D. + Psychiatric Residency)
- Psychiatric Nurse (LPN, BSN)
- Psychiatric Resident (M.D.)
- Psychiatric Social Worker (BSW, MSW, DSW)
- Psychometrist (M.A., M.Ed.)
- Psychotherapist (Varies)
- Recreational Therapist (A.D. or B.A./B.S.)
- Rehabilitation Counselor (Varies)
- Others: Alternative Medical Systems (Acupuncture, Chiropractor, Indigenous Healers, Naturopath, Shiatsu)
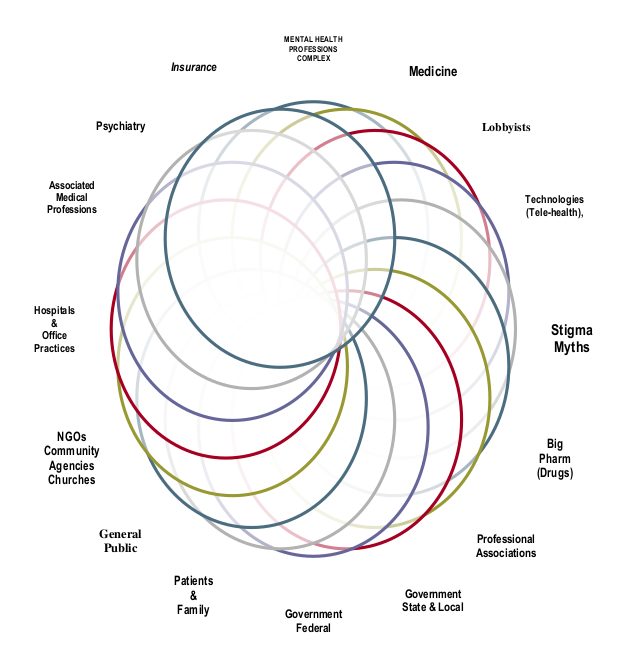
- The Ties that Bind
The mental health field is a web of inter-connected personal and professional relationships, ties, and obligations. Member critiques of each other risk condemnation and isolation.
Figure 1 displays the web of relationships. Does this web itself not become a source of problems for care facilitating preferred “evidence-based” approaches in mental health.
Figure 1: Web of MH Care-Systems Forces and Influences
- Reliance on a Flawed and Invalid Diagnostic and Classification System
It is now widely accepted, even among its supporters, that DSM systems from DSM I to DSM V is an anachronistic system traceable to historic and cultural forces and individual positions of power and influence. The subsequent emergence and empowerment of the DSM systems represent examples of the abuses of power and influence of conventional professions, individuals, groups, and, ultimately, government sanctioned (NIMH) and authority-figure assertions.
Figure 2 Displays “D” Word Alternatives Relative to Mental Health. The sheer variation and nuances of each category speaks to the awesome task of trying to arrive at reliable and valid diagnoses for purposes of therapy and counseling. What occurs is an informal or formal acceptance of various “D” words for purposes of work.
Figure 2: “D” Words and Mental Health (Marsella,2016)
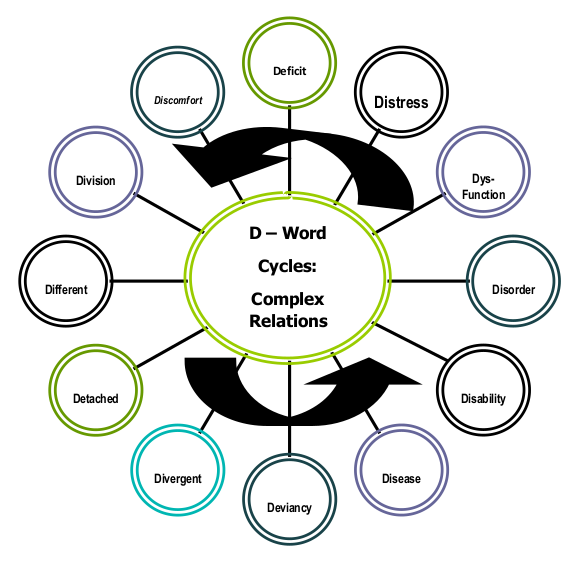
Consider this fact: Any of the “D” words constitute a dynamic patient state, subject to changes ranging from descriptors of their existence to subsequent interventions including precipitating factors, exacerbating factors, and maintaining factors. The idea of a static problem subject to distinct interventions does not exist.
The harsh reality is assignment to any “D” word category or diagnosis associated with a DSM system does not indicate: (1) Cause, (2) Symptom/Sign Display, (3) Site/Source of Pathology, (4) Course, (4) Outcome), (5) Treatment, or (6) Prevention. There are historic reasons for our continued use of the DSM, even as past adherents are seeking alternatives.
Compassion for mental health industrial-complex members is warranted; I nod my head amid the daily tasks before them. They are caught in a medical-political-economic-moral bind. Fixing the problem is beyond them, yet they are compelled to function amid the conventional system within which they work. I was there and made regret mistakes. My regret is no consolation for patients hurt by my decisions.
Concerns, Problems, Issues: Evidence-Based . . .
The primary problem, in my opinion, faced by evidence-based efforts is the failure to recognize the serious limitations in homogenized and standardize approaches and methods, and risks for care and healing.
Scientific and professional preferences for a canon fail to acknowledge the profound variations across each client, each therapist, each disorder(s), and each therapy and healing approach and method. There is an implicit insistence on uniformity at the expense of diversity and variation. This perpetuates myths of therapist, patient, therapy, and disorder in favor scientific and professional interests and concerns. This equation is displayed in Figure 2.
Figure 2: Equation of Determinants of Outcome for Psychotherapy and Counseling
Outcome = f constant x patient variability x therapist variability x disorder(s) x therapy methods x time x costs.
In addition, therapy and therapist availability, accessibility, and acceptability must be considered. The point being, homogenization of therapy is subject to considerable uniformity influences which deny variation.
Decades ago, Charles A. Kiesler, an eminent psychologist and university administrator, pointed out the myths of uniformity. He noted professional psychotherapy efforts fail to acknowledge ubiquitous variations in each of patients, therapists, methods, disorders (e.g., Kiesler, 1999).
The assertion of “empirically validated” therapies as the arbiter for implementation for “success,” “insurance,” and “conventional” acceptance is a serious challenge for therapists and healers of all identities.
Much of the assertion is based on clinical studies comparing therapies with controls. There are numerous problems with this strategy, and in my opinion, does not constitute a useful approach.
Among the typical problems from the point of view of valid and reliable research approaches are the following: (1) uniformity of patient samples; (2) fidelity of therapist interventions; (3) ethnocultural and racial identities of therapist and patient; (4) variations in disorders, dysfunctions, and deviancies; (5) confounding by past patient history including medical histories, diagnostic assignment using the problematic DSMIV and DSMV; (6) outcome measure limitations relying on simple ratings of scales by therapist or patient; (7) failure to consider ethnocultural variations in communication styles, appearance, language, and perceptions.
All of these considerations create extensive “error variance” which cannot be dismissed or processed via statistical procedures to highlight effects. Uses of different statistical methods can yield different results. Sample size may limit error, but it does not support minimal effects.
Outcome measures for evidence-based research too often fail to consider the spectrum of sources of patient reports including: (1) patient self-report (2) therapist evaluations; (3) family evaluations; (4) “objective” indicators of status; (5) institutional pressures for cure rates.
Existing conventional ‘in-group” advocates and supporters aligned with professional (APA) and scientific groups, are inclined to support notions of science associated with empiricism without considering the limitations of empiricism, especially inherent assumptions and preferred methods found among certain culturally-endorsed approaches (Marsella, 2009).
This speaks to the issues of “power” in professional and scientific groups, rather than doubt and contestation. There is a need here for reflexivity! “Power” in position does not yield easily; there is safety in convention. Cliques form in defense of particular theories, methods, and approaches claiming superiority (e.g., cognitive behavioral, psychodynamic, humanistic, behavioral).
Assuming a single therapy approach (e.g., Cognitive Behavior Therapy is current favorite) denies individual and cultural diversity and assumes application of the therapy method will be uniform across therapists. In addition, variations in the ethnocultural identity of therapist and client leads to considerable verbal and nonverbal communication problems.
Therapy outcome is a complex function of factors including the unique configuration of therapist, patient, disorder, therapy, time, cost, and healing principles.
As I studied, and applied different “Western” and “non-Western” therapies and counseling systems throughout my career, I concluded a number of “healing” principles exist; each is effective depending upon the uniqueness of each case, including the client characteristics, particular time in therapy cycle, situational considerations. Among these are the following:
- Beliefs (instill new beliefs or reinforce and reward others)
- Catharsis (anger, hate, fear, resentment)
- Confession
- Cultural re-embeddedness or cultural separation or cultural selective detachment
- Redefinition of problems
- Redefinition of self
- Empathy (communicate shared feeling and understanding)
- Expression and verbalization of problems
- Faith
- Forgiveness
- Hope
- Identity development and awareness
- Imagined and revenge
- Information exchange and enhancement
- Insight
- Interpretation of events
- Locus of control alterations
- Mobilization of endorphin and immune system (Thanks to Raymond Prince for this one)
- Propitiation
- Reduction of uncertainty, anxiety, fear through increase confidence and control
- Re-socialization and acquisition of new social skills
- Reduction of guilt and shame through approval and forgiveness
- Social supports and network development and strengthening
- Suggestion and persuasion
- Unconscious (making the unconscious conscious)
The point I wish to make is there are many ways to heal, and we should not be confined to a single approach or therapy model. No approach is best for all clients, all therapists, disorders, or situations. Uniformity risks error. For example, the widespread endorsement of cognitive behavior therapies may prove problematic. How does CBT work? Are there variations in CBT healing principles associated with CBT processes?
Further, there are many types of healers, and a one type of healer may not be best for everyone , or best for a situation in which there is a cultural difference.
Table 3: Examples of Traditional and Non-Western Health, Healers, and Therapy Systems (Marsella, 2010)
I – Examples of Traditional Healers/Therapists
- Curanderos (Latino)
- Dukhuns (Indonesia)
- Herbolarios & Hilots (Philippines)
- Kahunas (Hawaii)
- Mudangs (Korea)
- Santerias (Latino)
- Shamans (Widespread)
- Temple Masters and Priests (Buddhism, Taoism)
- Voudoo Trance Healers
II – Examples of Traditional Non-Western Health Systems
- American Indian
- Ayurveda (India, Hindu)
- East-Asian (Chinese Korean, Japanese, Tibetan)
- Indigenous (Australian Aboriginal, American Indian, Sub-
- Saharan Africa, Native Hawaiian and Pacific Island)
- Shamanistic Systems (World Wide)
- Unani (Arabic)
III – Examples of Traditional Non-Western Therapies
- Expressive Therapies (Art, Chanting, Dancing, Singing)
- Ho’oponopono (Hawaiian)
- I-Ching (Chinese)
- Meditation (Widespread)
- Morita Therapy (Japanese)
- Naikan Therapy (Japanese)
- Sweat Lodge/Vision Quest (American Indian)
- Voudoo (Caribbean/Africa)
- Yoga (India, Hindu)
Closing Thoughts
In a time and era when people of contrasting cultural diversity are coming into contact on a daily basis, it is incumbent dominant, historical, and conventional Western therapists and counselors learn the nature, procedures, and wisdom of traditional non-Western therapies, and in the process, re-consider the cultural context of their own practices.
Sensitivity to the cultural biases of their own systems is required as a first step in reducing potential abuses arising from good intentions being confused with potential problems in care and healing.
I am reminded of an ancient Chinese story of a monkey and a fish being caught in a turbulent flood.
The monkey and fish are being tossed in the waters and face a perilous end. The monkey then spies a branch and pulls himself out of the water; then wanting to help the fish, grabs the fish and holds the fish out of the water until the flood waters recede.
Moral: “Good intentions are not enough! “If you wish to help the fish, you must understand its nature.”
Do we understand the fish? The quest for uniform evidence-based treatments suggests to me there may be biases in failing to grasp the nature of mental health and therapies/ counseling. There is a need to be aware of the pressures for evidence-based interventions from insurance systems, professional organizations, and professional commitments to existing views of science, power, and position.
There are a number of things to be reconsidered:
- Views of human nature (Ontologies);
- Views of how we know what we know (Epistemologies);
- Views of our practices (Praxiologies);
- The nature and sources of our existing mental health industrial complex;
- The nature of the cultural construction of reality;
- The importance of wealth, power, position, and person in determining our actions (critical theory, paradigms)
REFERENCES:
Kiesler, C. A. (1966). Some myths of psychotherapy research and the search for a paradigm. Psychological Bulletin, 85, pp 110-136.
Marsella, A.J, (2009). Some reflections on potential abuses of psychology’s knowledge and practices. Psychological Studies, 1, 10-15. (Journal of the National Academy of Psychology – India)
Marsella, A.J., (2010). Ethnocultural aspects of PTSD: An overview of concepts, issues, and treatments. Traumatology, 16, 17-26.
Marsella, A.J. (2016). In pursuit of schizophrenia: Reflections on scientific and professional imprecision in thought and practice. Alpharetta, GA: Mountain Arbor Press. ISBN: 978-1—63183-037-2
Closing Coda
I enjoy Shakespearean writing genre. I often try to capture words and style for personal enjoyment. In the following example, I imagine an encounter between a Friar and a critic.
“And on what quaky foundation, pray tell me, stout friar, doeth thou continue to engage in acts of such pernicious consequence for human mind and spirit?
Art thou not uncomfortable with thy tasks? Fear thee not the risks of hell for those who feign claim sanctity in acts obvious to insult and to reason?”
“Tell me, friar, clothed, fed well, and filled in thy generous girth, with ale; art thou self-appointed in thy rounds, or given privilege by royal might?
Know paths thou tread are filled with unknown peril, springing from darkened places, products of thy own prior acts. Be alert to thy course! For in the presence of a stricken compass, choices become subject to destiny’s record.”
______________________________________
 Anthony J. Marsella, Ph.D., a member of the TRANSCEND Network for Peace Development Environment, is a past president of Psychologists for Social Responsibility, Emeritus Professor of psychology at the University of Hawaii’s Manoa Campus in Honolulu, Hawaii, and past director of the World Health Organization Psychiatric Research Center in Honolulu. He is known internationally as a pioneer figure in the study of culture and psychopathology who challenged the ethnocentrism and racial biases of many assumptions, theories, and practices in psychology and psychiatry. In more recent years, he has been writing and lecturing on peace and social justice. He has published 21 books and more than 300 articles, tech reports, and popular commentaries. His TMS articles may be accessed HERE and he can be reached at marsella@hawaii.edu.
Anthony J. Marsella, Ph.D., a member of the TRANSCEND Network for Peace Development Environment, is a past president of Psychologists for Social Responsibility, Emeritus Professor of psychology at the University of Hawaii’s Manoa Campus in Honolulu, Hawaii, and past director of the World Health Organization Psychiatric Research Center in Honolulu. He is known internationally as a pioneer figure in the study of culture and psychopathology who challenged the ethnocentrism and racial biases of many assumptions, theories, and practices in psychology and psychiatry. In more recent years, he has been writing and lecturing on peace and social justice. He has published 21 books and more than 300 articles, tech reports, and popular commentaries. His TMS articles may be accessed HERE and he can be reached at marsella@hawaii.edu.
This article originally appeared on Transcend Media Service (TMS) on 30 Apr 2018.
Anticopyright: Editorials and articles originated on TMS may be freely reprinted, disseminated, translated and used as background material, provided an acknowledgement and link to the source, TMS: Homogenization of Psychotherapy and Counseling: Scientific, Professional, Ethical/Moral Issues, Risks, and Directions, is included. Thank you.
If you enjoyed this article, please donate to TMS to join the growing list of TMS Supporters.
![]()
This work is licensed under a CC BY-NC 4.0 License.
Thanks for bringing this issue to the attention of the Transcend community. Brilliant and insightful!
Another home run for Tony. Pls publish
I have been retired for 8 years from the University of Hawai`i at Manoa where Tony Marsella also taught. Actually, I am now very angry at him for publishing this after I retired rather than before so that I could have used this piece in my classes. I am also angry at him for all the pieces of paper I used up printing his articled (11). Unfortunately for me and my former students, I see a little too much of myself in the homogeneity group, not enough in the, for want of a better term, the holistic group of educators and practitioners where decisions are more nuanced and less rigid and biased by a priori beliefs. Luckily for me (and my conscience), I am working on the seventh edition of a book where I can correct some of my misconceptions, and employ some of Tony’s ideas, some with proper credit, and maybe a couple that I pretend are my own.
This was a fabulous learning experience for me in the same sense that I used to define “learning experience” for my students: any cognitive experience that is painful and difficult.
I am gravely concerned that rural people in the US and elsewhere do not have enough mental health practitioners. I am genuinely concerned that today’s practitioners are not able to treat today’s problems.