
On the Dialectic between Social Processes and Health/Illness Processes
EDITORIAL, 1 Jun 2020
#641 | Johan Galtung - TRANSCEND Media Service
[From TMS Editor: An editorial from Johan Galtung a bit longer and older but with contemporary relevance. From the context of the 1980’s HIV-AIDS pandemic, Galtung offers unique insights into the hurdles and challenges humanity faces today with COVID-19.]
[This text has been transcribed and could contain typographical errors. Please refer to original PDF here.]
*************************
November 1982
The general approach taken in this paper is not only that social formations of different types generate their own patterns of health and disease, but also that these patterns work on the social formations in a complex interactive relationship. Much of this is spelt out in the chart on the next page; what follows here is a translation into hopefully more readable language of what is contained in that chart.
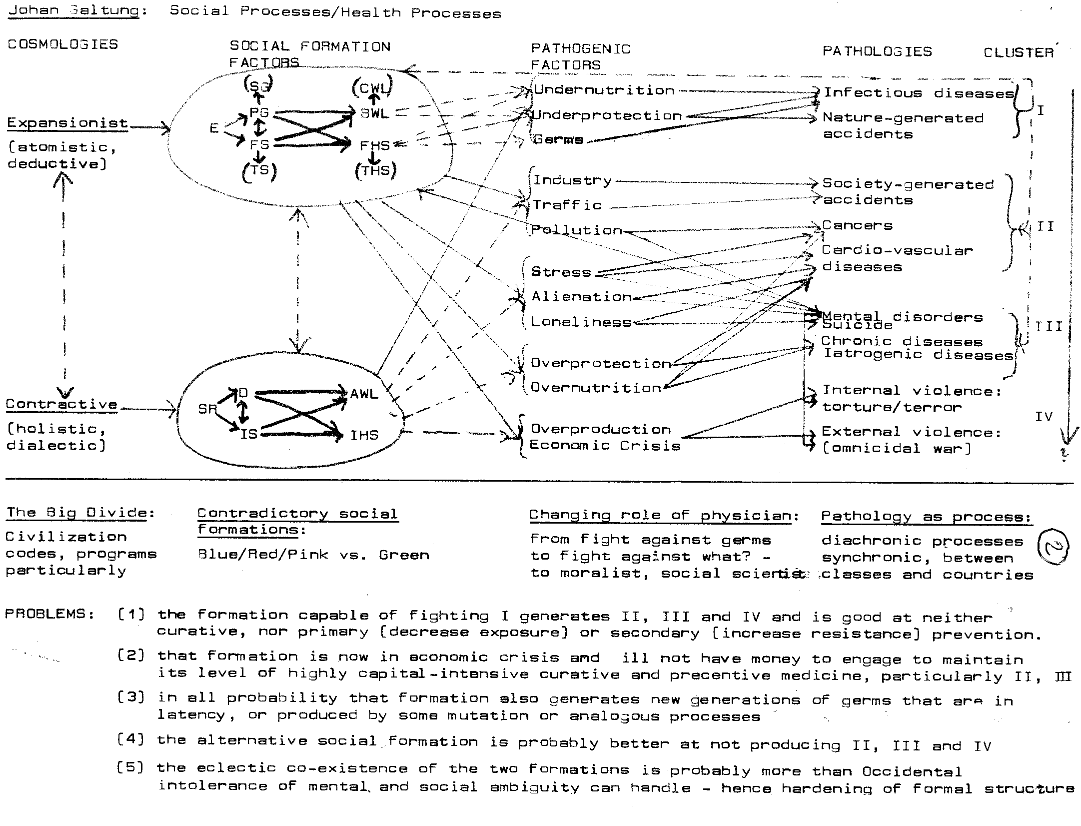
Let me start on the right hand side, with the pathologies, meaning any state of the human being, body, mind and/or spirit, considered incompatible with the WHO definition of health as “a sense of well-being”. They are organized into four clusters.
The Classification is not logical but to some extent sociological: the general hypothesis is that each cluster relates to aspects of a social formation. However, social formations may coexist, in any given society several there may be leads and lags in the social processes, meaning that the clusters can very well overlap in time.
Cluster I contains the classical diseases, infectious diseases and nature generated accidents. We tend to see them as the kind of diseases common to human beings in a relatively primitive or traditional existence, with a low level of mastery of nature. Humans become easy preys of germs and natural hazards; of the atmosphere such as hurricanes, hydrosphere such as tsunamis; floods and drought; of the and of the lithosphere such as wild-fires, volcanoes, earth-quakes. I am not necessarily accepting that perspective. If “mastery” in a western sense” is interpreted as “technical mastery, then the perspective may be valid, even fruitful. But there may also be other types of mastery, perhaps less occidental, perhaps unknown to us whereby ability to coexist with germs and with nature may be higher. Some day we might also discover that human beings are not only the victims of germs and accidents generated by nature but also, perhaps, their catalysts with the propensity for awakening sleeping dogs, even at a low level of technical civilization. However, be that as it may: cluster I is certainly what is associated with the relatively recent past of industrialized society and the present as experienced by very many people in non-industrialized countries.
The second cluster of diseases changes the focus: disease is now seen as more generated by society and not only through accidents but also in the form of the two big killers, cardio-vascular diseases and cancers. Again, the perspective engendered by the term “civilization diseases” is problematical. Such diseases certainly have occurred in all kinds of societies, only “civilized” ones. Moreover, not to relate the diseases to “civilization” – a very broad term – is not only to prejudge the issue but also to put a mental stop in front of further research. The pathogenic factors might be located in some aspects of some civilizations, but the term indicates that this will apply to all civilizations, perhaps also to very many aspects of them.
The third cluster is of a very different kind. One might imagine a society where cluster I has been, practically speaking, eliminated through strategies of primary and secondary prevention, and cluster II made compatible with a quite high life expectancy. Just as the longevity produced by practically speaking eliminating cluster I yields a population with a high incidence of cancers and cardio-vascular diseases, a curative approach to the latter – these are diseases that touch the human body profoundly – will tend to leave the society with a population very high on chronic diseases. A population of that kind will have an extended and deep contact surface with the health community in general and doctors in particular, and this will increase the incidence of iatrogenic diseases. Finally, because of other aspects of this social formation that currently is the most prevalent in the world, the western social formation, high incidence of mental disorders, especially the lighter forms, and also suicide might be expected.
The fourth cluster is of a different kind: it refers to internal and external violence as major forms of pathologies, certainly maiming, even destroying, the human body, mind and spirit. The very existence of Red-Cross, military medical services in peace and particularly in war give ample testimony to the fact that one is dealing here with some type of pathology. To the adherents of the theory of innate human aggressiveness these may be referred to as “nature generated accidents”; to the more sociologically oriented school in the study of human violence, they might be seen as “society generated accidents”. Of course such dichotomies should yield in favor of more dialectic approaches looking for changing interaction patterns between nature and society.
Here they are seen as pathologies in their own right because of the alarming proportion they have attained recently, both in the internal form of terrorism, torture and government supported killing of undesirable political opposition and because of the threat felt in so many parts of the world today of a war of mass destruction, particularly with nuclear weapons. And there seems also to be general consensus that curative medicine is totally inappropriate, particularly as the formal health structure itself will be destroyed, (FHS) built up for this purpose that secondary prevention (increasing the resistance to wars of mass destruction particularly through civil defense) is doomed to be inefficient relative to such insults, so that the only way out is primary prevention, trying to eliminate the exposure, meaning the threat of a war of mass destruction. Health professions in particular, and the western social formation in general, had success with cluster I: both primary and secondary prevention have been highly successful so that there is less of a need for the curative approach that, incidentally, still is remarkably unsuccessful relative to the more dangerous epidemics. And it differs also from the second cluster where the curative approach is making advances even at a relatively quick pace and what would constitute primary and secondary prevention: at least, they are known, even if not fully to some extent, engaged in.
It is more similar, however, to what can be found in connection with the third cluster. By definition the curative approach is unsuccessful (otherwise the diseases would not have taken on their chronic character); no very clear formula for secondary prevention seems to exist, psyche simply being vulnerable, human bodies and the human leaving us with primary prevention, with less exposure of us humans to pathogenic factors. In short, the transition from clusters I and II towards clusters III and IV is a transition towards decreasing reliance on curative approaches and increasing necessity of engaging in primary prevention.
Or, at least, that is what it looks like today – leaving open the possibility that in some years, generations, decades, the picture may look entirely different. The question arises, why is this so?
In one sentence: because we are moving into types of diseases more and more deeply related to a social formation itself in processes of growth, change and decay; very difficult to steer or control. We may be on top of the germs, or at least of many germs; but the society and its processes, or at least most of it, indeed, seems to be on top of us. But these are global expressions so let us try to make it more specific by talking in terms of social formation factors, and pathogenic factors.
The western social formation is here seen in terms of five factors: A general pattern of exploitation of the internal proletariat, (of other countries, of nature and eventually of everybody including the exploiters), (PG) a heavy emphasis on production and growth and the creation of a formal sector
(FS) based on planning-oriented bureaucracies, market-oriented corporations and abstraction-oriented intelligentsia with professional skills; the two of them together contributing to a bourgeois way of life (BWL) – non-manual work, material comfort, high level of privatization and search for security and a formal health sector (FHS) gradually monopolizing tasks in primary and secondary preventive medicine and curative medicine.
The history of the success of this general formation in combating cluster I of diseases has been considerably clarified through the important research tradition symbolized by the name of McKeown. The bourgeois way of life became gradually the way of life for substantial segments of the population in the countries practicing the western social formation, including its exploitative aspects. As a result under-nutrition yielded, and under-protection relative to the hazards of nature went away and with it the exposure of the human body to excessively cold and moist or hot and moist environments, nutrition, settings in which particular germs became particularly lethal.
The synergistic effect of under-nutrition, under-protection and germs continues making its terrible toll on populations in countries with other social formations or with insufficient proportions of the population inside the protective cocoon of that formation. All three aspects have to be attacked, not only the germs, not only the under-protection, not only the under-nutrition. One may then dispute which factor is most or least important, often a misleading discussion because of the synergistic nature of the phenomenon.
But it worked, as evidenced very clearly by the health statistics in the world. However, that very western social formation, so successful in combating cluster I had in it some aspects themselves pathogenic factors for pathologies not unknown qualitatively but certainly unencountered quantitatively outside western social formations. Here they are referred to as “industry”, “traffic”, “pollution”. The human-made environment in which industrial work unfolded itself for the proletariat, if not for the considerably more protected management, the urban environment in which modern means of traffic became a major factor together with the general pollution of atmosphere, hydrosphere and biosphere expose human beings to something hitherto unknown. It is no longer a question merely of temperature and degree of humidity, or of more dramatic hazards of nature: the hazards are brought into the working place and the living place themselves. No primitive society would knowingly put up their dwellings on top of a volcano; knowingly, “modern” human beings put that volcano, inside their factories and cities. The pathology equation between environment and human beings changes with well known consequences. As the pathogenic factors increase in strength they make their toll also on less worn out, aging human beings, perhaps marked by having been “successfully” through a couple of cluster I diseases: increasingly cluster II is being felt among the young, even among children. Traffic accidents already have a relatively clear structure: the middle aged killing the young and the old; males killing females. But these are highly concrete phenomena; a dangerous machine in a factory is highly visible, so is a car speeding where children are crossing. Pollutants in air and water, milk in plants and animals, in mother’s are neither visible nor audible. Merely to detect them is a pain-staking process, knowledge about them has to be mediated, primary and secondary prevention does not have the automatism of a person trying to avoid car accidents. Hence, more professionalism!
Much of this has to do with the exploitation of nature, of creating a nature no longer capable of absorbing and degrading pollutants toxic to human beings. And much of it has to do with the exploitation of the internal proletariat: the accidents caused by industry usually have a very clear class structure, just like the accidents caused by traffic have a clear age and gender structure.
Correspondingly the diseases of the third cluster relate to the exploitation of Self: the focus is now on a society pressing its members into levels of achievement through structures so formalized, so non-human that the result cannot help being the synergistic operation of stress, alienation and loneliness. At the same time the effort to provide all members of society with the bourgeois way of life has become so effective that over-protection and over-nutrition (or perhaps rather mal-protection and malnutrition in some cases) are the results, combining with all the other factors in producing clusters II and III diseases.
Schematically one can say that for each generation or clusters of diseases the western social formation as depicted in the diagram has to pay for one or more of its patterns of exploitation. In the first cluster it was particularly the internal proletariat that had to pay because of its low level of resistance due to the exposure to natural hazards when living in a surrounding of under-nutrition and under-protection. In the second cluster it is the exploitation of nature that hits back in the form of pollution together with the exploitation of everybody in the form of stress, and over-protection.
This exploitation of everybody is also over-nutrition prevalent in the third cluster of diseases, operating through structures that dehumanize people through excessive division of labour,
fragmentation (splitting of people away from each other), segmentation (splitting of people inside themselves, making them live “segmentally”, thing then, doing one thing now, never leading a more integrated life) and above all with considerable vertical distance between top and bottom. This does not mean, incidentally, that only the bottom suffers: the BCI complex is structured in such a way that both parts suffer through the inhuman social environment.
Then the fourth type of exploitation really hits back: exploitation of the external sector. This is then seen as a major cause, among several, of external war – just as internal exploitation is seen as the major cause of internal wars, ultimately resulting in terrorism from below and torture combined with government sponsored murder from above. Exploitation of an external sector means making other countries reservoirs for raw nature, raw labour and raw (uncommitted) capital as well as markets for one’s own products. The whole history of the socialist revolution from 1917 and the rise of the “Third World” from 1945 is the history of countries that no longer wanted to play that role. How that in turn leads to the east-west conflict and the rapidly upcoming north-south conflict also in belligerent terms (the Falkland/Malvinas war possibly being the first good example where north had an ideal enemy to fight against) is long and complex and not to be elaborated here. But the basic point is again the same: each social formation generates the threat to the human body and mind and spirit that is rooted in the deeper layers of its structures and processes. That this ultimately can lead to “the white death”, extinction in the lightning of nuclear warfare, is obvious and not to be elaborated here.
What is very interesting in this context, however, is to look at the arrows in the opposite direction. Something has been said how about now social formations generate certain diseases; what can be said about diseases as causal factors, among others, in generating social formations? Usually the problem is not put that way since diseases are seen as dependent, not as independent variables.
And yet it is obvious that, as often pointed out, a population with very low life expectancy suffering from acute and chronic contagious diseases is not a population capable of sustained economic growth, in other words, of carrying out the program of the western social formation. It is a population that dies too young to gain sufficient experience, also a population too decimated and emaciated by disease to have sufficient stamina to generate new efforts in production and growth. It is a population that becomes hesitant and stagnant, better at preserving old traditions. Concretely this means that just as the western social formation through the bourgeois way of life and the formal health structure is able to protect its population against contagious diseases, grosso modo, the opposite is also true: a population with higher life expectancy and lower levels of mortality in general is more capable of building that social formation.
But from this rather trivial observation what, then, follows as we pursue the pattern downwards through the diagram? What kind of social formation will come out of clusters II and III, perhaps combined rather than singly? We are then dealing with a population considerably older on the average, eventually going to die like in any other population but increasingly so from a disease family with a very bad reputation as a cruel, often slow and very often very painful killer: malignant tumors. In other words the quality of life generated through the effective fight against cluster I is mitigated by the decreasing quality of death generated by cluster II if one accepts the image of a death from cancer as inferior in quality to most deaths from contagious diseases. Moreover, particularly when cluster III is taken into consideration one may also question the quality of life, particularly in. the second half or the last third of the life span. It is marked by a high incidence of chronic diseases that earlier, perhaps, were overshadowed by a higher threshold of tolerance and masked by earlier death. The same may apply to mental disorders, necessarily in the heavier forms (schizophrenia, not psychoses) but in the heavy increase in the lighter forms (neuroses). In other words, a population living not in conscious happiness because it is relieved of the scourges of parents and grandparents, but in the highly conscious anxiety of the threat that may already be working inside their bodies, cancers, and incapacitated by the synergistic workings of chronic diseases and mental disorders. How will a population of that kind react?
Difficult to say. But one guess, and a rather important one, may be that just as the social formation generates in increasing proportion mental disorders (although of the lighter kinds) people affected by such disorders may also serve to strengthen that social formation in a particular and obnoxious way. A definition of mental disorder may then be needed: I see them as conditions that make people significantly less able to live together with other people, to handle inter-human and social affairs.
This may come so far that the social response is institutionalization, in other words marginalization, some kind of exile. But it may also go in another direction and a much more threatening one. There is another way of escaping from inter-human relations one cannot handle: into the worlds and words of abstraction, particularly into formal social structures, be those in the state bureaucracies or the capitalist corporations or both. Instead of dealing with people one deals with symbols, with papers, with abstractions people are at the distance and appear only as statistics, symbols, objects without face and names. From this the step is not very far from what is indicated in the diagram, formal structure to totalitarian structure (TS), from characterized not only by a much higher level of integration between state and capital and professions (the BCI complex), but also by even more distance between ruler and ruled so that dehumanization is even more effectively built into the structure that then becomes an even more ideal abode for mentally deranged people. And at this point they become dangerous: with that distance people become the easy objects not only of manipulation, but also of extinction. Personally I find it difficult to explain or understand in a deeper sense the horrors of the twentieth century (and we still have two decades to go!) only in terms of normal people who obediently do their jobs within authoritarian structures. I feel this image is an insult to our concept of human beings. After all few animals take such a long time to grow up and for that reason are in need of such a long period of at least some type of compassion between parents and offspring and for that reason, in turn, have such a potential for empathy and compassion. I think one also needs to see here the interplay between mental disorder in the sense indicated above and the distance created by gigantic, all-encompassing, formal structures.
However, in order to maintain a structure of that type more than conventional production and growth will be needed. The system demands some type of supergrowth (SG). One sees the contours of that type of production system today, even more dehumanized, robotized, highly automated, with adjustment of people to the products rather than vice versa. And one also sees the impact of this in the bourgeois way of life, the transformation towards a “chemical/circus way of life” (CWL), characterized by ever increasing intakes of alcohol and other drugs, of tobacco, coffee, and other stimulants; tea eventually also sugar and salt, of chemically treated food with natural fibres removed and a spectator oriented, highly sedentary life – epitomized by the legendary TV-watcher, in front of his TV-set with a drink, he needs to smoke, firmly planted ample supply of what and junk food. A form of life which in itself assures for him and her a future replete with cluster II and III diseases, and premature death.
Finally, the response of all of this in the formal health sector: of course moves towards a totalitarian health sector (THS). There are two reasons for this. First, it is the obvious reflection of a transition from the classical formal structure to a more totalitarian structure, which is now emerging, in the field of health. It will take the forms of an ever more integrated cooperation between central bureaucratic administration, health industries and the health professions, of expertise and power, a seamless web impenetrable from the outside. The distance to the patient will increase, diagnosis may be by remote sensing, a urine test analyzed through information channels connected with the telephone/TV/radio system, and so on. And the second reason is also simple: since a lower and lower proportion of the population given the increasing prevalence of cluster III will be what could be called healthy, higher and higher numbers will have to be diagnosed and treated one way or the other so that the “productivity” simply has to increase. Just as for other problems generated by this formation the answer will be, in all probability, as indicated.
I take this to be our likely future in the coming ten to fifteen years. Of course there are counter-trends and they fill up the bottom left hand part of the diagram. It is an alternative social formation, certainly non-western in the current phase of western history, not necessarily found in clear shape in any part of the highly westernized world in which we live. Rather than exploitation its point of departure is self reliance; go soft on nature; cooperation between. labour buyers and labour sellers in small cooperatives; relatively modest productivity, making use of one’s own resources before one tries to get at others through trade; trade only when this is impossible and when the trade can be with other countries at the same level of technical development so that center periphery gradients are avoided. The system generates less material goods, but what it generates one then attempts to distribute more evenly with a particular emphasis on the satisfaction of basic needs for the bottom parts of the population. The structures are kept at a more local level, state formation is modest, such is national market formation, informal structures among families, friends, in villages and communes are dominant, not recessive features of the social order. This is then expressed in an informal health structure which is characterized by a high level of self-cure, mutual cure, other cure and a diversity of traditional medicines of various types. And as to the general way of life: an effort to combine manual and non-manual work rather than a striving to only have the latter; an effort to have a minimum of material protection against the more extreme hazards but otherwise live not only in closeness but also in harmony — with nature; an effort to live together with others, more collectively rather than in the private retreat of ever smaller family systems; and an effort to lead a less preordained, perhaps more unpredictable, more varied way of life rather than to obtain security at the expense of monotony. In short, some kind of mixture of are seen as traditional, pre-capitalist, movement, and social forms that often in European history sometimes as some of it found in the green wave and so and so forth.
The problems with this are two-fold. The first problem has to do with health/disease theory: although it may be strongly argued that a social formation of this kind is so much softer, so non-exploitative that clusters IV will be less dominant, II, III and it is hard to argue that it is capable of combating cluster I diseases at the level of efficiency we are used to today. One might argue that one could then settle for a higher level of contagious diseases if with that one could avoid clusters II, III and IV. But the goal of our health systems is not in that direction; it is towards eradication and with considerable justification. Hence, the question rather becomes whether one could try to develop the formal health structure and the pillars on which it rests only to the point that is necessary and sufficient for this goal to be obtained, not further. In other words, could one imagine, a limitation to the minimum, maybe more concentrated on the work of sanitation engineers, hygiene experts in general, and the social and political work needed to raise the levels of nutrition and protection of the underprivileged in these two fields? It might certainly be argued that by means of that one could relatively simply reap a very solid harvest in terms of decreasing cluster I diseases. And it might be argued that one could even identify in the health processes of certain First World countries what was the optimum point: in Norway, perhaps, the latter half of the 1960s where we perhaps passed that optimum without knowing it since we did not know where we were heading – and correspondingly for other countries within this social formation.
But then comes the second problem. This is not only a question of health and disease, it is a question of very far reaching and deep social, political, economic and ultimately cultural concerns. One may even go so far as to say that the fight between the western social formation and the alternative one is the basic political fight today, being fought all over the world. It is only in some First World countries that there is some sympathy for the alternative social formation because many people have seen the limitations of the dominant one. In the Second World, the socialist countries, there is an almost unambiguous dedication to the goals of the First World, only with a much higher emphasis on the state sector and less on the capital sector in the capitalist sense. the Third World one finds the same: In “development” is indeed defined as the fight against this alternative social formation in an effort to imitate the western one on one’s own soil. In fact, as indicated in the diagram, the whole alternative social formation is antagonistic to the western social formation even if so many of the adherents are the products of that very formation. Any transition towards the alternative formation means a loss of power and prestige for those on the top of the mainstream formation. And any halt in the transition of Third World countries that still have substantial elements of the “green” alternative will mean less of the promised land for those who believe in the western social formation with the fervor that is only possible when one is not oneself a member.
In short: politics. And behind that politics deeply rooted social programs, codes or cosmologies – vaguely hinted at to the left in the diagram. With more ability to think and act so as to try to combine what seems uncombinable there might be less of a problem: one could try and build a society in-between, trying to locate an optimum with features of both without using the alternative sector in a perverted form as a reservoir for the lower classes and the marginalized – a trend found all over the world today. But precisely that ability to combine the uncombinable is itself a victim of the process called “modernization”, making the situation even more difficult.
Hence, now, it looks as if the Third World is doomed, right to live through the chapters of health/illness history as witnessed by the West – in short that he who does not know history is bound to relive it. Or, is there some other way out that might also give some fresh approaches to the societies well into clusters II and III?
__________________________________________
 Johan Galtung, a professor of peace studies, dr hc mult, is founder of TRANSCEND International and rector of TRANSCEND Peace University. He was awarded among others the 1987 Right Livelihood Award, known as the Alternative Nobel Peace Prize. Galtung has mediated in over 150 conflicts in more than 150 countries, and written more than 170 books on peace and related issues, 96 as the sole author. More than 40 have been translated to other languages, including 50 Years-100 Peace and Conflict Perspectives published by TRANSCEND University Press. His book, Transcend and Transform, was translated to 25 languages. He has published more than 1700 articles and book chapters and over 500 Editorials for TRANSCEND Media Service. More information about Prof. Galtung and all of his publications can be found at transcend.org/galtung.
Johan Galtung, a professor of peace studies, dr hc mult, is founder of TRANSCEND International and rector of TRANSCEND Peace University. He was awarded among others the 1987 Right Livelihood Award, known as the Alternative Nobel Peace Prize. Galtung has mediated in over 150 conflicts in more than 150 countries, and written more than 170 books on peace and related issues, 96 as the sole author. More than 40 have been translated to other languages, including 50 Years-100 Peace and Conflict Perspectives published by TRANSCEND University Press. His book, Transcend and Transform, was translated to 25 languages. He has published more than 1700 articles and book chapters and over 500 Editorials for TRANSCEND Media Service. More information about Prof. Galtung and all of his publications can be found at transcend.org/galtung.
Tags: AIDS, COVID-19, Coronavirus, HIV, Health, Pandemic, Public Health, Social conflict, Social sciences
This article originally appeared on Transcend Media Service (TMS) on 1 Jun 2020.
Anticopyright: Editorials and articles originated on TMS may be freely reprinted, disseminated, translated and used as background material, provided an acknowledgement and link to the source, TMS: On the Dialectic between Social Processes and Health/Illness Processes, is included. Thank you.
If you enjoyed this article, please donate to TMS to join the growing list of TMS Supporters.
![]()
This work is licensed under a CC BY-NC 4.0 License.
What a wonderful idea to reprint this thoughtful and far-seeing article just at this time! As we (in the “rich world) look around and wonder if we have learnt anything over the centuries about how to deal effectively with “plagues”, with relations between nations, with food production and distribution, with obesity, diabetes and other lifestyle factors overpowering our national health systems (or lack of them, in the USA!). Many now have noticed the reduced pollution, the needless consumerism, the ability to do many jobs themselves, the encroachment of nature, just in a few weeks of forced confinement. Surely our way of life needs to be adjusted to be in some sort of harmony, but it is with our own human characteristics we need to find a balance, as the “control” of nature has its limits.
Thanks, as always, to dear Johan Galtung and TMS.